
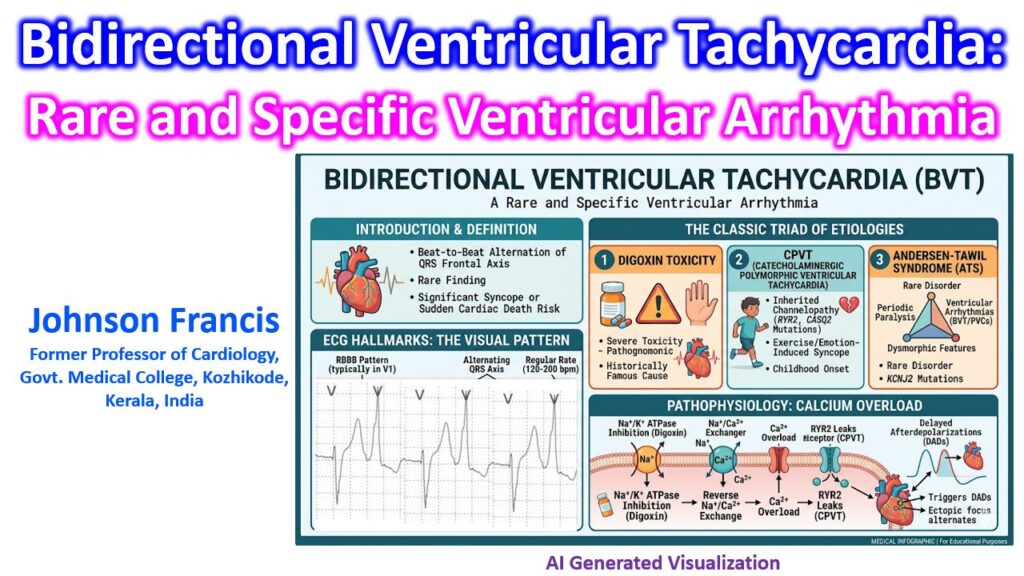

Bidirectional Ventricular Tachycardia (BVT) is a rare, highly specific ventricular tachyarrhythmia characterized by a beat-to-beat alternation of the QRS frontal plane axis. It is a critical finding when evaluating syncope or sudden cardiac death, particularly in patients with structurally normal hearts.
ECG Hallmarks
The diagnosis hinges on clear pattern recognition:
- Heart Rate: Typically ranges between 120 and 200 bpm.
- Morphology: Usually presents with a Right Bundle Branch Block (RBBB) pattern in lead V1.
- The “Bidirectional” Feature: A beat-to-beat alternation of the QRS axis in the limb leads (alternating between left axis deviation and right axis deviation).
The “Classic Triad” of Etiologies
If BVT appears on a monitor, the differential diagnosis is incredibly narrow and should immediately trigger consideration of three primary conditions:
- Digitalis Toxicity: Historically the most famous cause. BVT in a patient on digoxin is considered pathognomonic for severe toxicity until proven otherwise.
- Catecholaminergic Polymorphic Ventricular Tachycardia (CPVT): An inherited channelopathy—most commonly an autosomal dominant mutation in the RYR2 gene, or autosomal recessive in CASQ2. It presents with exercise- or emotion-induced syncope, often starting in childhood.
- Andersen-Tawil Syndrome (ATS): A rare disorder linked to KCNJ2 mutations (Kir2.1 channel). It classically presents with the triad of periodic paralysis, ventricular arrhythmias (including BVT or frequent PVCs), and dysmorphic physical features.
(Rare outliers include aconite poisoning, severe myocarditis, or familial hypokalemic periodic paralysis).
Pathophysiology: The Calcium Overload
The underlying electrophysiological mechanism unifying these distinct etiologies is intracellular calcium overload leading to delayed afterdepolarizations (DADs).
- In Digoxin Toxicity: Inhibition of the Na+/K+ ATPase pump leads to increased intracellular Na+. This reverses the Na+/Ca2+ exchanger, flooding the cell with calcium.
- In CPVT: The mutated ryanodine receptor (RYR2) becomes “leaky” during sympathetic stimulation (catecholamine release), spontaneously releasing Ca2+ from the sarcoplasmic reticulum during diastole.
When these DADs reach threshold, they trigger ectopic beats. The characteristic “alternating axis” is thought to occur because the ectopic focus alternates between the anterior and posterior fascicles of the left bundle branch (or alternatively, firing from alternating sites in the left and right ventricles).