

Yes, unequivocally. Heart rate recovery (HRR) is a powerful, independent predictor of all-cause and cardiovascular mortality. Here is a breakdown of the clinical evidence, the physiology, and how we measure it.
The Physiology: Vagal Reactivation
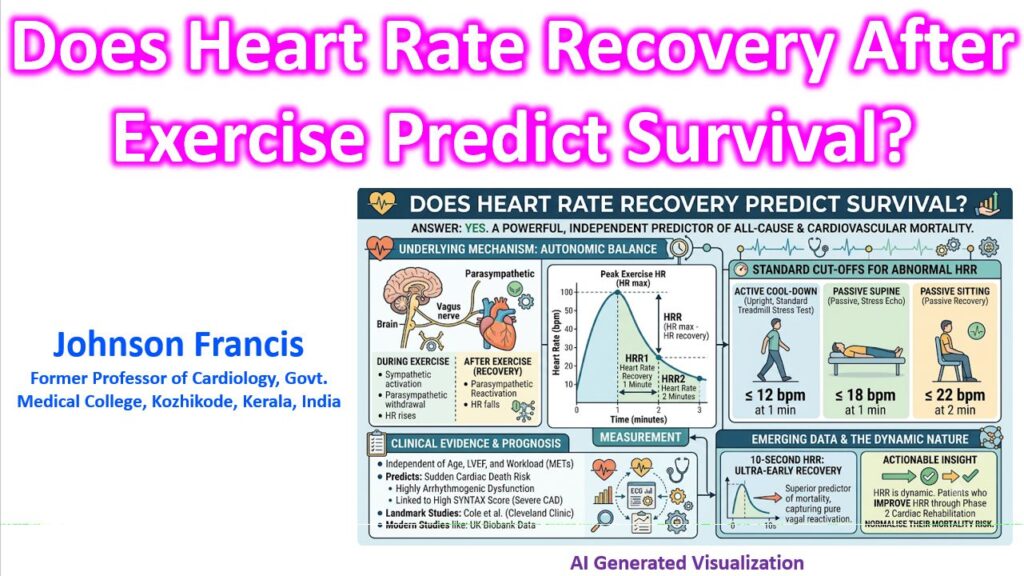
Heart rate during exercise is driven by sympathetic activation and parasympathetic withdrawal. Once exercise stops, the immediate drop in heart rate is primarily driven by parasympathetic (vagal) reactivation, not just sympathetic withdrawal.
An abnormally slow heart rate recovery indicates autonomic dysfunction—specifically, blunted vagal tone. Because diminished vagal tone is highly arrhythmogenic and associated with a higher risk of ventricular fibrillation and sudden cardiac death, a delayed HRR serves as a red flag for cardiovascular vulnerability.
Standard Cut-offs for Abnormal HRR
HRR is calculated by subtracting the heart rate at a specific time in recovery from the peak heart rate achieved during stress testing. The cut-offs for what is considered “abnormal” depend entirely on the patient’s position and activity level during the recovery phase:
- Upright (Active Cool-down): ≤ 12 bpm drop at 1 minute. (Typical for standard treadmill stress tests).
- Supine (Passive Recovery): ≤ 18 bpm drop at 1 minute. (Typical for stress echocardiography where the patient immediately lies down).
- Sitting (Passive Recovery): ≤ 22 bpm drop at 2 minutes.
The Clinical Evidence
The prognostic power of HRR is well-established, tracing back to landmark data from the Cleveland Clinic, which demonstrated that an abnormal HRR is predictive of death independent of the angiographic severity of coronary artery disease (CAD).
- Independent of LVEF and Workload: HRR predicts mortality even after adjusting for age, left ventricular ejection fraction, standard risk factors, and total exercise capacity (METs).
- Predicts High SYNTAX Scores: More recent data links a blunted HRR to a significantly higher likelihood of having severe, complex CAD (SYNTAX score ≥ 23).
- The 10-Second Window: While 1-minute HRR is the clinical standard, recent large-cohort studies (like those utilizing UK Biobank data) suggest that ultra-early recovery—specifically the HR drop at 10 seconds post-exercise—might be an even superior predictor of mortality, as it most purely captures the initial spike of parasympathetic reactivation.
Key clinical takeaway: HRR is dynamic. Studies have shown that patients with an abnormal HRR at baseline who undergo phase 2 cardiac rehabilitation and normalize their HRR see their mortality risk drop back to the level of patients who had a normal HRR from the start.