

The primary limiting factor for exercise is almost always the underlying structural heart disease in a person with optimized pacing system, rather than the presence of the device itself. Assuming the patient has a structurally normal heart (e.g., isolated congenital heart block or pure sick sinus syndrome), they can participate in running with virtually no restrictions. Situation may be different in a person with a single-chamber non-rate responsive pacemaker. However, to ensure a patient can run safely and asymptomatically, several programming and structural parameters must be optimized even in those with the better pacing system.
Hemodynamic Programming
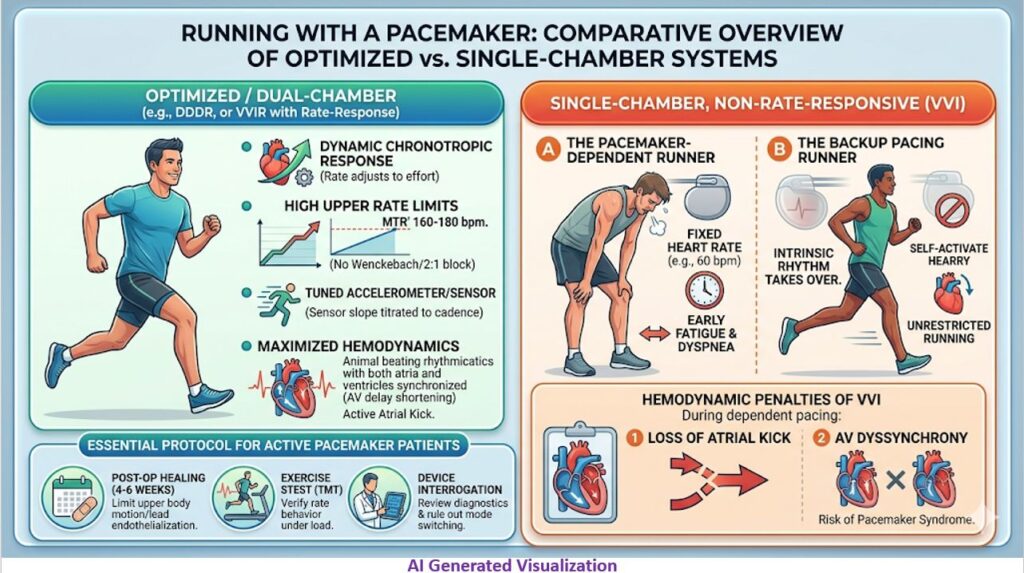
The most common cause of exercise intolerance in a runner with a pacemaker is suboptimal programming, specifically regarding upper rate behaviors.
- Maximum Tracking Rate (MTR) / Upper Sensor Rate (USR): The MTR must be programmed sufficiently high to accommodate the target heart rate during a run. If a patient’s atrial rate exceeds the MTR, the device will exhibit pacemaker Wenckebach or suddenly drop into a 2:1 block. This sudden drop in the ventricular paced rate causes a precipitous fall in cardiac output and acute dyspnea. For young or highly active runners, the MTR may need to be pushed to 160–180 bpm, depending on the device’s limit and the patient’s age-predicted maximum.
- Rate-Responsive Sensor Tuning: For patients relying on the device for chronotropic competence, the sensor (accelerometer or minute-ventilation) must be optimized. Running provides excellent mechanical feedback for accelerometers, but the slope and threshold must be titrated so the pacing rate rises appropriately with the run’s cadence and decays smoothly during recovery.
- AV Delay Algorithms: Dynamic or rate-adaptive AV delays should be enabled to mimic the physiologic shortening of the PR interval during tachycardia, which optimizes diastolic filling times at high heart rates.
Structural and Lead Considerations
While running is a non-contact sport—meaning direct trauma to the generator is exceptionally rare—the biomechanics of running still present structural variables.
- Post-Implant Healing: Patients are universally advised to avoid vigorous upper-body movement and heavy exertion for the first 4 to 6 weeks post-implantation. This allows for adequate pocket healing and lead endothelialization, mitigating the risk of micro-dislodgement.
- Lead Stress: Repetitive arm swing during long-distance running creates continuous, low-grade mechanical stress on the leads. While lead fracture is more common in sports requiring extreme shoulder mobility (like swimming or tennis), chronic friction can increase the risk of subclavian crush syndrome over the lifetime of a highly active athlete. This is particularly relevant if the lead was placed via a medial subclavian puncture rather than a cephalic cutdown.
- Leadless Pacemakers: For highly active runners, leadless systems are increasingly favored. By sitting entirely within the right ventricle, they completely eliminate the risks of lead fracture, subclavian crush, and pocket-related complications from repetitive motion.
Clinical Evaluation
Before clearing a patient for distance running or high-intensity interval training (HIIT), a standard clinical evaluation usually includes:
- Exercise Stress Test (TMT): This is critical to evaluate the patient’s intrinsic chronotropic response, rule out exercise-induced ischemia, and verify that the pacemaker’s MTR and rate-response profiles are behaving hemodynamically as intended under actual physical load.
- Device Interrogation: Reviewing diagnostic data post-run ensures there are no inappropriate mode switches (e.g., sinus tachycardia misclassified as an atrial tachyarrhythmia) and monitors for any exercise-induced ventricular ectopy.
Single-chamber, non-rate-responsive pacemaker (VVI or AAI)
Running with a single-chamber, non-rate-responsive pacemaker (VVI or AAI) is physically possible, but the hemodynamic experience depends entirely on how dependent the patient is on the device during exertion. Because the pacemaker lacks both an atrial lead to track intrinsic sinus tachycardia and a sensor (the “R” in VVIR) to detect physical movement, it cannot artificially accelerate the heart rate.
The Pacemaker-Dependent Patient
If the patient relies on the VVI device for every beat (e.g., chronic complete AV block or permanent atrial fibrillation with complete AV node ablation), running will be extremely difficult.
- Fixed Heart Rate: The ventricular rate remains locked at the programmed lower rate limit (e.g., 60 or 70 bpm).
- Stroke Volume Ceiling: Because Cardiac Output = Heart Rate × Stroke Volume, and the heart rate cannot increase, the body must rely entirely on stroke volume augmentation to meet the metabolic demands of running.
- Clinical Presentation: Stroke volume alone is severely insufficient for aerobic exercise. The patient will hit a strict physiologic “wall” almost immediately, experiencing profound early fatigue, dyspnea, heavy legs, and potentially presyncope due to chronotropic incompetence.
The “Backup” Pacing Patient
If the pacemaker is implanted primarily for intermittent symptomatic bradycardia (e.g., paroxysmal AV block, intermittent sinus pauses, or neurocardiogenic syncope), the patient can often run with zero restrictions.
During exertion, normal sympathetic drive takes over. The intrinsic sinus node accelerates, the AV node conducts (if intact), and the pacemaker simply senses the intrinsic rhythm and appropriately inhibits itself. In this ideal scenario, the pacemaker is essentially a dormant safety net while the patient’s natural conduction handles the run.
The Hemodynamic Penalty of VVI
Even if a patient can run, VVI pacing carries inherent structural disadvantages during exercise compared to dual-chamber systems:
- Loss of Atrial Kick: VVI pacing causes AV dyssynchrony. The loss of coordinated atrial contraction eliminates the “atrial kick,” which normally contributes 20–30% of left ventricular end-diastolic volume. During running, when filling times are shortened and preload augmentation is critical, this loss significantly blunts maximum stroke volume.
- Risk of Pacemaker Syndrome: If the patient has intact retrograde ventriculoatrial (VA) conduction, ventricular pacing can force the atria to contract against closed AV valves. This causes cannon A waves, raises right atrial pressures, and directly impairs forward cardiac output, actively working against the athlete during a run.
If a patient with a non-rate-responsive VVI device is highly motivated to run but is limited by chronotropic incompetence, the definitive clinical solution is upgrading the system to enable rate-responsiveness (VVIR) or placing an atrial lead to restore AV synchrony and allow tracking of the intrinsic sinus node.