
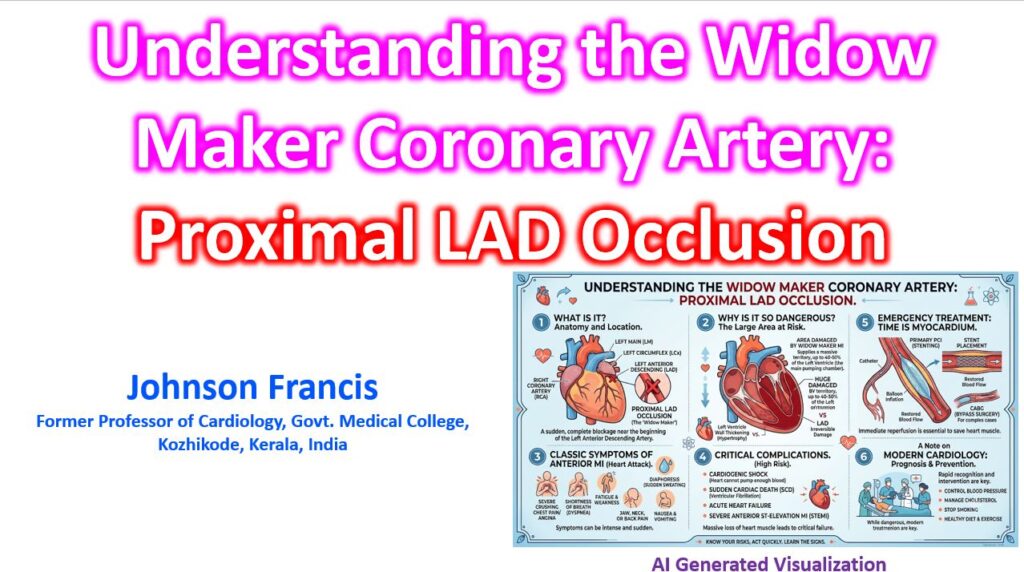

The term “widow maker” is the colloquial, though clinically ominous, name given to a critical stenosis or massive occlusion of the proximal Left Anterior Descending (LAD) artery. Because the LAD supplies a massive proportion of the left ventricular myocardium, an acute occlusion at its origin—before it gives off major septal and diagonal branches—places the patient at an extremely high risk for catastrophic outcomes like cardiogenic shock, fatal arrhythmias, or rapid structural failure.
Here is a breakdown of the clinical and anatomical nuances that make proximal LAD lesions so critical.
Anatomical Territory at Risk
The LAD is the largest and most crucial of the coronary arteries. It typically arises from the left main coronary artery and courses down the anterior interventricular sulcus. A proximal occlusion threatens a massive territory:
- Anterior Wall of the Left Ventricle: Supplied by the diagonal branches (D1, D2, etc.). Loss of this territory rapidly degrades Left Ventricular Ejection Fraction (LVEF).
- Anterior Two-Thirds of the Interventricular Septum: Supplied by the septal perforators. This houses the bundle branches; ischemia here frequently leads to conduction blocks (e.g., right bundle branch block with a left anterior fascicular block).
- Apex: Often supplied entirely by the LAD, though sometimes shared depending on whether the vessel “wraps around” the apex (a “wrap-around LAD”).
If the occlusion is proximal to the first septal perforator (S1) and first diagonal (D1), the entire anterior wall and most of the septum are starved of oxygen simultaneously.
Classic ECG Presentations
While an acute anterior STEMI is the most obvious presentation, a proximal LAD lesion often tips its hand through specific, high-risk ECG patterns before full infarction occurs.
- Anterior STEMI: ST-segment elevation in the precordial leads (V1-V6), often with reciprocal ST depression in the inferior leads (II, III, aVF).
- Wellens’ Syndrome: A critical warning sign of a highly stenotic LAD that has transiently reperfused. It presents as deeply inverted or biphasic T-waves in V2 and V3 during a pain-free interval. If missed, it frequently progresses to an extensive anterior STEMI within days.
- De Winter’s T Waves: An anterior STEMI equivalent signifying acute proximal LAD occlusion. Look for ST-segment depression at the J-point (1-3 mm) in anterior leads, continuing into tall, prominent, symmetrical T-waves, without classic ST elevation.
Clinical Management and Prognosis
The term “widow maker” originated before the era of primary Percutaneous Coronary Intervention (PCI). Today, rapid revascularization drastically changes the prognosis, but the stakes remain the highest of any single-vessel occlusion.
- Intervention: Emergent PCI is the standard of care for an acute occlusion. However, if a severe proximal LAD stenosis is found during angiography alongside complex multivessel disease—especially in diabetic patients or those with a reduced LVEF—Coronary Artery Bypass Grafting (CABG) utilizing the Left Internal Mammary Artery (LIMA) to the LAD remains the gold standard for long-term survival.
- Complications: Even with successful reperfusion, patients are at high risk for acute complications like ventricular fibrillation, and subacute complications like left ventricular aneurysm formation or mural thrombus due to apical akinesis.