

Atrial fibrillation (AFib) with rapid ventricular response (RVR) is a cardiac arrhythmia characterized by completely disorganized electrical activity in the heart’s upper chambers (atria) combined with a fast, irregular response from the lower chambers (ventricles). Clinically, it presents as an “irregularly irregular” heart rhythm with a resting ventricular rate typically exceeding 100 beats per minute (often ranging between 120 and 160+ bpm).
The Mechanism
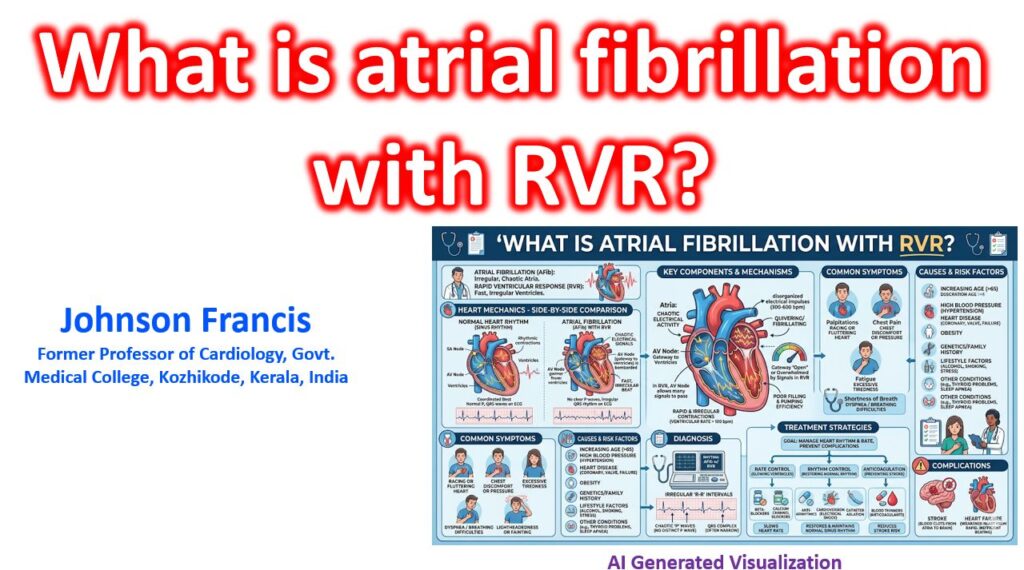
To understand RVR, it helps to look at the interaction between the atria and the atrioventricular (AV) node:
- The Fibrillating Atria: In AFib, the heart’s normal pacemaker (the SA node) is overridden by multiple chaotic, micro-reentrant electrical circuits. Instead of a unified contraction, the atria quiver, generating electrical impulses at a blistering rate of 300 to 600 times per minute. This eliminates distinct P-waves on an ECG.
- The AV Node as Gatekeeper: These hundreds of signals bombard the AV node, the electrical gateway to the ventricles. The AV node’s natural refractory period protects the lower chambers by blocking the vast majority of these impulses.
- The Rapid Ventricular Response: In RVR, the AV node allows a higher percentage of these disorganized impulses to pass through. Because the signals arrive at the AV node randomly, the resulting ventricular contractions (the QRS complexes) occur at completely unpredictable intervals, creating the classic irregular pulse.
Clinical Consequences
A heart beating rapidly and irregularly struggles to pump blood efficiently, leading to several physiological challenges:
- Decreased Cardiac Output: The rapid rate severely shortens the diastolic phase — the split-second when the heart relaxes and fills with blood. If the ventricles don’t have enough time to fill, stroke volume (the amount of blood pumped per beat) drops significantly.
- Loss of “Atrial Kick”: Because the atria are quivering rather than squeezing, the heart loses its final, active push of blood into the ventricles. This loss reduces overall ventricular filling by another 20-30%.
- Symptom Cascade: The combination of poor filling and high oxygen demand can trigger palpitations, shortness of breath, lightheadedness, hypotension, or even acute decompensated heart failure and myocardial ischemia if the coronary arteries can’t keep up with the heart’s oxygen needs.
Clinical management of Atrial Fibrillation (AFib) with Rapid Ventricular Response (RVR)
The clinical management of Atrial Fibrillation (AFib) with Rapid Ventricular Response (RVR) hinges on a rapid assessment of hemodynamic stability, followed by a structured approach to rate control, rhythm control, and stroke prevention. Here is a breakdown of the standard clinical protocols.
1. Initial Assessment: Hemodynamic Stability
The immediate triage branching point is determining if the rapid ventricular rate is severely compromising cardiac output.
- Hemodynamically Unstable: Signs include hypotension, altered mental status, signs of shock, ischemic chest discomfort, or acute heart failure.
- Action: Immediate synchronized electrical cardioversion. Delaying for pharmacological interventions is not recommended when perfusion is critically compromised.
- Hemodynamically Stable: The focus shifts to slowing the ventricular rate, evaluating the need for rhythm control, and assessing thromboembolic risk.
2. Acute Rate Control
For stable patients, the primary goal is to increase the AV node refractory period to slow the ventricular response, typically targeting a resting heart rate of < 110 bpm (lenient control) or < 80 bpm (strict control for symptomatic patients). Drug selection depends heavily on the patient’s Left Ventricular Ejection Fraction (LVEF) and comorbidities.
Pharmacological Options
| Drug Class | Examples | Clinical Considerations |
| Beta-Blockers | Metoprolol, Esmolol (IV) | Highly effective; first-line for most patients. Caution in reactive airway disease or decompensated heart failure. |
| Non-DHP CCBs | Diltiazem, Verapamil (IV) | Excellent rate control. Strictly contraindicated in patients with HFrEF (systolic dysfunction) due to negative inotropic effects. |
| Cardiac Glycosides | Digoxin (IV/PO) | Useful as an adjunct or in patients with HFrEF and borderline blood pressure. Slower onset of action compared to beta-blockers or CCBs. |
| Antiarrhythmics | Amiodarone (IV) | Used for rate control primarily in critically ill patients or those with severe HFrEF when other agents are ineffective or contraindicated. |
3. Rhythm Control vs. Rate Control
While rate control is the initial acute step, deciding whether to actively restore and maintain normal sinus rhythm (NSR) is a longer-term strategy.
- Favor Rhythm Control: Younger patients, highly symptomatic individuals despite adequate rate control, newly diagnosed/first-episode AFib, or patients with tachycardia-induced cardiomyopathy.
- Methods: Electrical cardioversion, pharmacological cardioversion (e.g., Flecainide, Propafenone, Amiodarone, Ibutilide), or catheter ablation (pulmonary vein isolation).
- Favor Rate Control: Older, asymptomatic patients, or those with long-standing persistent AFib where maintaining sinus rhythm is unlikely to be successful.
The 48-Hour Rule: If initiating rhythm control (especially cardioversion) and the onset of AFib is > 48 hours or unknown, a transesophageal echocardiogram (TEE) must be performed to rule out a left atrial appendage (LAA) thrombus, or the patient must be therapeutically anticoagulated for at least 3 weeks prior.
4. Stroke Prevention (Anticoagulation)
AFib causes blood stasis in the atria, significantly increasing the risk of thromboembolism and ischemic stroke. Anticoagulation strategy is dictated by risk stratification, not by whether the patient is in a rate or rhythm control pathway.
- Risk Stratification: Use the CHA2DS2-VASc score to estimate annual stroke risk.
- Score 0 (males) or 1 (females): Anticoagulation generally not recommended.
- Score 1 (males) or 2 (females): Consider anticoagulation.
- Score ≥ 2 (males) or ≥ 3 (females): Oral anticoagulation strongly recommended.
- Agent Selection:
- Direct Oral Anticoagulants (DOACs): Apixaban, Rivaroxaban, Dabigatran, Edoxaban. These are the preferred agents for non-valvular AFib due to a favorable efficacy-to-bleeding profile and lack of routine monitoring requirements.
- Vitamin K Antagonists (Warfarin): Required for patients with moderate-to-severe mitral stenosis or mechanical heart valves.
5. Long-Term Optimization (The “ABC” Pathway)
Comprehensive management follows the Atrial fibrillation Better Care (ABC) pathway:
C – Cardiovascular and Comorbidity optimization: Aggressively managing underlying triggers such as hypertension, obesity, obstructive sleep apnea, diabetes, and heart failure to reduce the atrial substrate for fibrillation.
A – Anticoagulation/Avoid stroke: Continuous risk assessment.
B – Better symptom management: Ongoing adjustments to rate/rhythm therapies.