


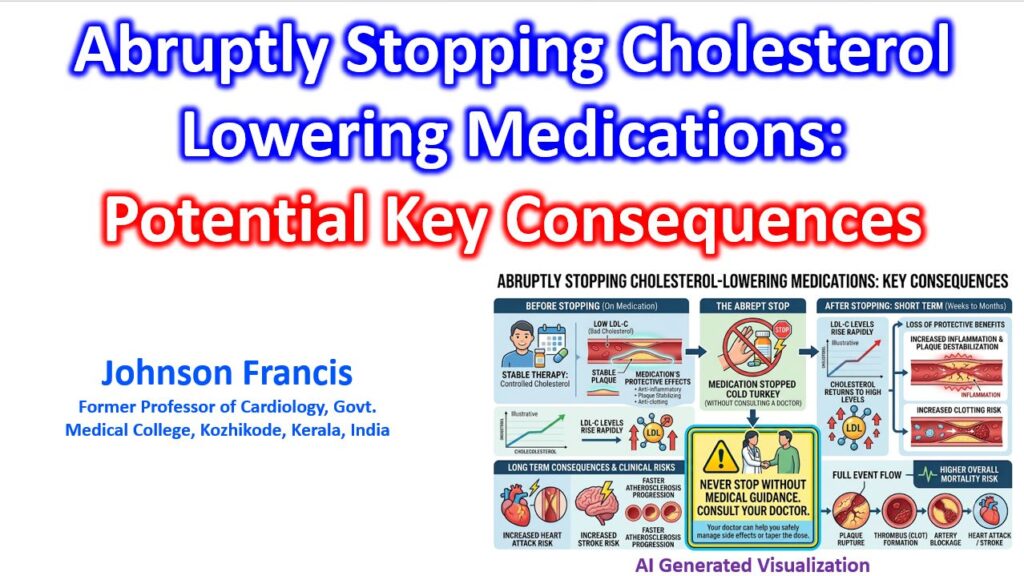

When a patient abruptly discontinues lipid-lowering therapy—specifically statins—the clinical outcome is dictated less by the gradual return of circulating cholesterol, and more by an acute pleiotropic rebound (a sudden loss of the drug’s lipid-independent, anti-inflammatory stabilizing effects on the vascular wall).
While a stable primary prevention patient with clear vessels might simply revert to their baseline lipid curve over a few weeks, an individual with established atherosclerotic disease enters an immediate, highly volatile window of plaque destabilization.
The Pathophysiology of the Rebound Overshoot
When intracellular statin concentrations drop to zero, the sudden unblocking of the mevalonate pathway triggers an overshoot in the production of downstream isoprenoids (lipid intermediates like farnesyl pyrophosphate that anchor signaling proteins to cell membranes). This sets off a rapid cascade of adverse vascular mechanics:
- The Rho/ROCK Activation Spike: The sudden glut of isoprenoids causes an extreme over-activation of Rho-associated protein kinase (ROCK). This drives acute vascular smooth muscle contraction, spikes local reactive oxygen species, and suppresses endothelial nitric oxide synthase (the enzyme responsible for generating vasodilatory nitric oxide), instantly shifting the endothelium into a vasoconstrictive, pro-thrombotic state.
- Enzymatic Cap Degradation: Within days of withdrawal, activated macrophages inside the atheroma ramp up the transcription of matrix metalloproteinases (enzymes that degrade collagen and the extracellular matrix). This rapidly thins the protective fibrous cap overlying the lipid core.
- Platelet Hyper-reactivity: The sudden loss of statin-mediated tissue factor suppression prompts an uptick in circulating thromboxane A2 production. If the newly thinned fibrous cap suffers even a microscopic fissure, local rheology strongly favors immediate, occlusive thrombus propagation.
- Receptor Re-equilibration: Systemically, the hepatic upregulation (the compensatory increase in cell-surface receptor density) of LDL receptors reverses within 14 to 21 days, returning circulating serum ApoB and LDL-C back to their pre-treatment baseline.
Clinical Risk Stratification
Because this rebound phenomenon strikes the micro-environment of the vessel wall long before a standard serum lipid panel reflects the change, the clinical danger of stopping cold-turkey scales entirely with the patient’s underlying vascular anatomy:
| Clinical Setting | Immediate Hazard (0–30 Days) | Long-Term Trajectory |
| Stable Primary Prevention | Negligible acute risk; serum lipids normalize within 2 to 4 weeks. | Gradual return to the patient’s baseline lifetime atherosclerotic risk curve. |
| Stable Chronic CAD | Subclinical spike in vascular inflammation and subtle endothelial dysfunction. | Accelerated expansion of existing necrotic cores and a higher 1-year MACE risk. |
| Acute Coronary Syndrome (ACS) | Severe risk of acute cap rupture, target lesion thrombosis, or fatal re-infarction. | Markedly elevated 90-day mortality (historically doubled compared to maintained therapy). |
Key Insight: The hazard of abrupt statin cessation in an unstable vessel is a classic biological paradox: the drug successfully quieted the inflammatory cross-talk of the atheroma, but withdrawing it acts as a cellular stress test, handing the inflammatory momentum right back to the vulnerable plaque.
References
Giral P, Neumann A, Weill A, Coste J. Cardiovascular effect of discontinuing statins for primary prevention at the age of 75 years: a nationwide population-based cohort study in France. Eur Heart J. 2019 Nov 14;40(43):3516-3525. doi: 10.1093/eurheartj/ehz458. PMID: 31362307; PMCID: PMC6855142.
Jeong HY, Lee SY, Kim SH, Kim J. Long-Term Benefit and Withdrawal Effect of Statins After Percutaneous Coronary Intervention: A Nationwide Population-Based Cohort Study. Patient Prefer Adherence. 2020 Apr 5;14:717-724. doi: 10.2147/PPA.S245324. PMID: 32308376; PMCID: PMC7147626.
Lee SH, Kwon HS, Park YM, Ko SH, Choi YH, Yoon KH, Ahn YB. Statin Discontinuation after Achieving a Target Low Density Lipoprotein Cholesterol Level in Type 2 Diabetic Patients without Cardiovascular Disease: A Randomized Controlled Study. Diabetes Metab J. 2014 Feb;38(1):64-73. doi: 10.4093/dmj.2014.38.1.64. Epub 2014 Feb 19. PMID: 24627830; PMCID: PMC3950197.