



Acute Pulmonary Embolism (PE) remains a critical diagnosis requiring rapid risk stratification to dictate management, particularly in the era of expanding catheter-directed therapies and advanced hemodynamic support.
Risk Stratification and Initial Assessment
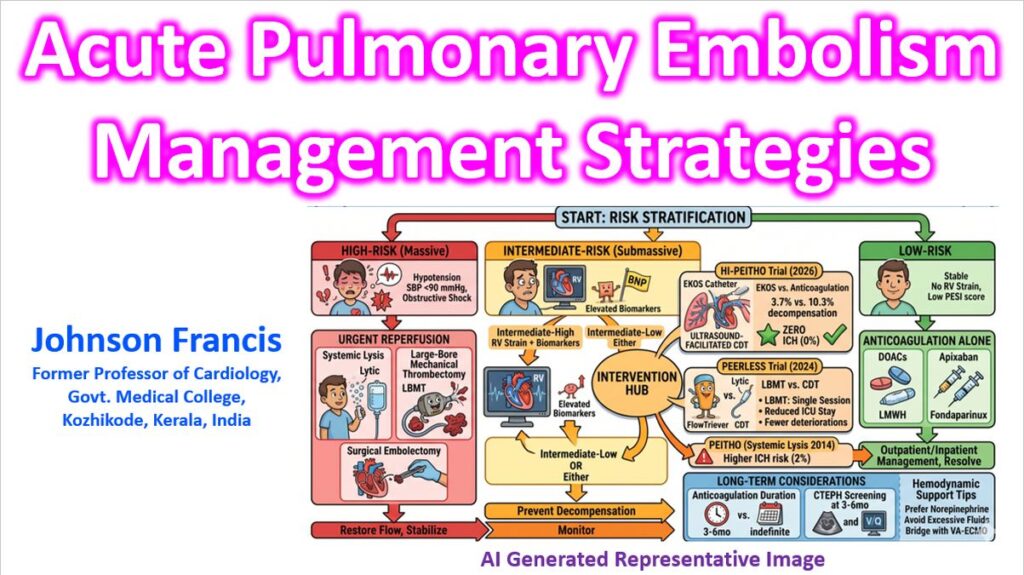
The immediate priority is determining hemodynamic stability, as this bifurcates the entire diagnostic and therapeutic algorithm.
- High-Risk (Massive) PE: Defined by sustained hypotension (SBP <90 mmHg for >15 min), obstructive shock, or the need for inotropic support.
- Intermediate-Risk (Submassive) PE: Hemodynamically stable but shows evidence of right ventricular (RV) strain.
- Intermediate-High: Both elevated cardiac biomarkers (Troponin, BNP) and RV dysfunction on imaging (Echo or CT).
- Intermediate-Low: Either elevated biomarkers or RV dysfunction, but not both.
- Low-Risk PE: Hemodynamically stable with no signs of RV strain and low scores on clinical prediction rules (PESI/sPESI).
Diagnostic Workup
For stable patients, the YEARS algorithm approach is standard to reduce unnecessary CT Pulmonary Angiograms (CTPA). YEARS clinical decision rule consists of three items – clinical signs of deep vein thrombosis, haemoptysis, and whether pulmonary embolism is the most likely diagnosis. These along with D-dimer concentration can be used to assess need for CTPA. In patients without YEARS items and D-dimer less than 1000 ng/mL, or in patients with one or more YEARS items and D-dimer less than 500 ng/mL, pulmonary embolism was considered excluded. All other patients need CTPA.
| Diagnostic Tool | Clinical Utility |
| CTPA | The gold standard for anatomical confirmation and assessing the RV/LV ratio (ratio >0.9–1.0 indicates strain). |
| Bedside Echo | Critical for unstable patients; look for McConnell’s Sign, 60/60 sign, or right heart thrombus (thrombus-in-transit). |
| V/Q Scan | Preferred in patients with renal failure or severe contrast allergy. |
| Compression Ultrasound (CUS) | Useful when CTPA is unavailable; a positive DVT in a symptomatic patient is often sufficient to initiate treatment. |
Management Strategies
1. Anticoagulation
Immediate initiation of anticoagulation (unless contraindicated) is mandatory.
- LMWH/Fondaparinux: Generally preferred over UFH in stable patients due to more predictable pharmacokinetics.
- Unfractionated Heparin (UFH): Preferred in high-risk patients, those with severe renal impairment (CrCl <30 mL/min), or when immediate reversal/surgery is anticipated.
- DOACs: Now the first-line therapy for long-term management in most stable patients.
2. Reperfusion Therapy
- Systemic Thrombolysis: Indicated for High-Risk PE. Tenecteplase or Alteplase are standard. Half-dose thrombolysis is often considered in intermediate-high risk cases with a high bleeding risk, though evidence remains nuanced.
- Catheter-Directed Thrombolysis (CDT): Increasingly used for Intermediate-High Risk patients to provide localized thrombolysis with significantly lower systemic bleeding risks.
- Mechanical Thrombectomy: Indicated for high-risk patients where thrombolysis is contraindicated or has failed. Large-bore aspiration systems have shown high efficacy in clot burden reduction.
- Surgical Embolectomy: Reserved for patients with contraindications to thrombolysis or those with “clot-in-transit” through a patent foramen ovale (PFO).
3. Hemodynamic Support
In the setting of RV failure, aggressive fluid resuscitation can be counterproductive by worsening RV dilation and causing the interventricular septum to shift, further reducing LV preload.
- Vasopressors: Norepinephrine is generally first-line to maintain systemic MAP and coronary perfusion to the RV.
- ECMO: VA-ECMO serves as a bridge to recovery or intervention in patients with refractory cardiogenic shock.
Long-Term Considerations
- Provoked vs. Unprovoked: This distinction determines the duration of anticoagulation (3–6 months vs. indefinite).
- CTEPH Screening: Patients with persistent dyspnea 3–6 months post-PE should be screened for Chronic Thromboembolic Pulmonary Hypertension (CTEPH) via Echo and V/Q scan.
The management of intermediate-high risk (submassive) pulmonary embolism has undergone a paradigm shift with the release of recent landmark trial data. For years, clinicians operated in a “gray zone” between the high bleeding risks of systemic thrombolysis (ST) seen in the PEITHO trial and the conservative approach of anticoagulation alone. Recent data, specifically from the HI-PEITHO trial, now provides high-level evidence supporting catheter-based interventions as a first-line strategy for these patients.
Landmark Clinical Trial Data
1. HI-PEITHO: Ultrasound-Facilitated CDT vs. Anticoagulation
Presented at the American College of Cardiology (ACC) 2026 Annual Session and simultaneously published in The New England Journal of Medicine, the HI-PEITHO trial is now the definitive reference for catheter-directed thrombolysis (CDT) in intermediate-risk PE.
- Study Design: Randomized 544 patients with intermediate-risk PE and signs of clinical severity (tachycardia, low BP, or hypoxia) to ultrasound-facilitated CDT (EKOS system) plus anticoagulation vs. anticoagulation alone.
- Primary Endpoint: A 7-day composite of PE-related mortality, cardiorespiratory collapse, or symptomatic PE recurrence.
- Results: The EKOS group showed a 61% reduction in the primary endpoint (4.0% vs. 10.3%; P=0.005). This benefit was largely driven by a significant reduction in cardiorespiratory decompensation.
- Safety Profile: Crucially, there were zero (0%) intracranial hemorrhages in the EKOS arm through 30 days, addressing the primary safety concern associated with the original PEITHO (systemic lysis) trial.
2. PEERLESS: Mechanical Thrombectomy vs. CDT
While HI-PEITHO established CDT over anticoagulation, the PEERLESS trial compared two different interventional modalities: Large-Bore Mechanical Thrombectomy (LBMT) and CDT (Jaber et al., 2024).
- Findings: LBMT (using the FlowTriever system) was found superior to CDT based on a 5-component hierarchical win ratio.
- Key Drivers: The superiority was primarily due to lower rates of clinical deterioration and significantly reduced ICU utilization (41.6% for LBMT vs. 98.6% for CDT).
- Clinical Takeaway: LBMT provides a “single-session” resolution without the need for an ICU stay for drug infusion, though safety outcomes (mortality/major bleeding) were similar between both interventional groups.
2026 AHA/ACC Guideline Updates
The 2026 Guideline for the Evaluation and Management of Acute Pulmonary Embolism in Adults has introduced a new classification system to refine treatment selection with 5 categories (A-E) and subcategories, ranging from low to high risk for adverse outcomes.
- Category C (Elevated Risk): Patients with RV strain and biomarker elevation but stable hemodynamics. The guidelines now suggest consideration of catheter-based therapies (CDT or LBMT) as an early intervention for those with high clot burden or worsening respiratory status.
- Category D (Incipient Failure): Patients who are technically stable but show “soft” signs of failure (e.g., lactate elevation, persistent tachycardia). These patients are now primary candidates for interventional reperfusion to prevent the 10.3% collapse rate seen in the conservative arms of recent trials.
Category A is subclinical while Category B is symptomatic with low clinical severity score. Category E is cardiopulmonary failure.
Comparative Evidence Summary
| Feature | Systemic Thrombolysis (PEITHO 2014) | Catheter-Directed (HI-PEITHO 2026) | Mechanical (PEERLESS 2024) |
| Dose | 100 mg Alteplase (Full dose) | ~16–20 mg Alteplase (Local) | Zero Lytic |
| ICH Risk | ~2.0% | 0.0% | 0.7% |
| Primary Benefit | Prevented decompensation | Prevented decompensation | Reduced ICU stay & deterioration |
| ICU Necessity | Mandatory | Mandatory (for infusion) | Often unnecessary |
Ongoing Research: Pulmonary Embolism: Thrombus Removal with Catheter-Directed Therapy (PE-TRACT)
The PE-TRACT study is currently following patients with intermediate-risk pulmonary embolism for up to 12 months to determine if early CDT improves long-term functional status and exercise capacity . Results are expected to further refine the “Lytic-free” vs. “Ultra-low-dose Lytic” debate.
References
2026 Guideline for the Evaluation and Management of Acute Pulmonary Embolism in Adults. Circulation.
Jaber, W. A., Gonsalves, C. F., Stortecky, S., et al. (2024). Large-Bore Mechanical Thrombectomy Versus Catheter-Directed Thrombolysis in the Management of Intermediate-Risk Pulmonary Embolism: Primary Results of the PEERLESS Randomized Controlled Trial.
Konstantinides, S. V., et al. (2026). Ultrasound-facilitated Catheter-directed Thrombolysis vs. Anticoagulation Alone in Intermediate-Risk Pulmonary Embolism: The HI-PEITHO Randomized Trial. The New England Journal of Medicine.
Meyer, G., Vicaut, E., Danays, T., et al. (2014). Fibrinolysis for patients with intermediate-risk pulmonary embolism. The New England Journal of Medicine, 370(15), 1402–1411.