Biatrial enlargement on CXR
Biatrial enlargement on CXR
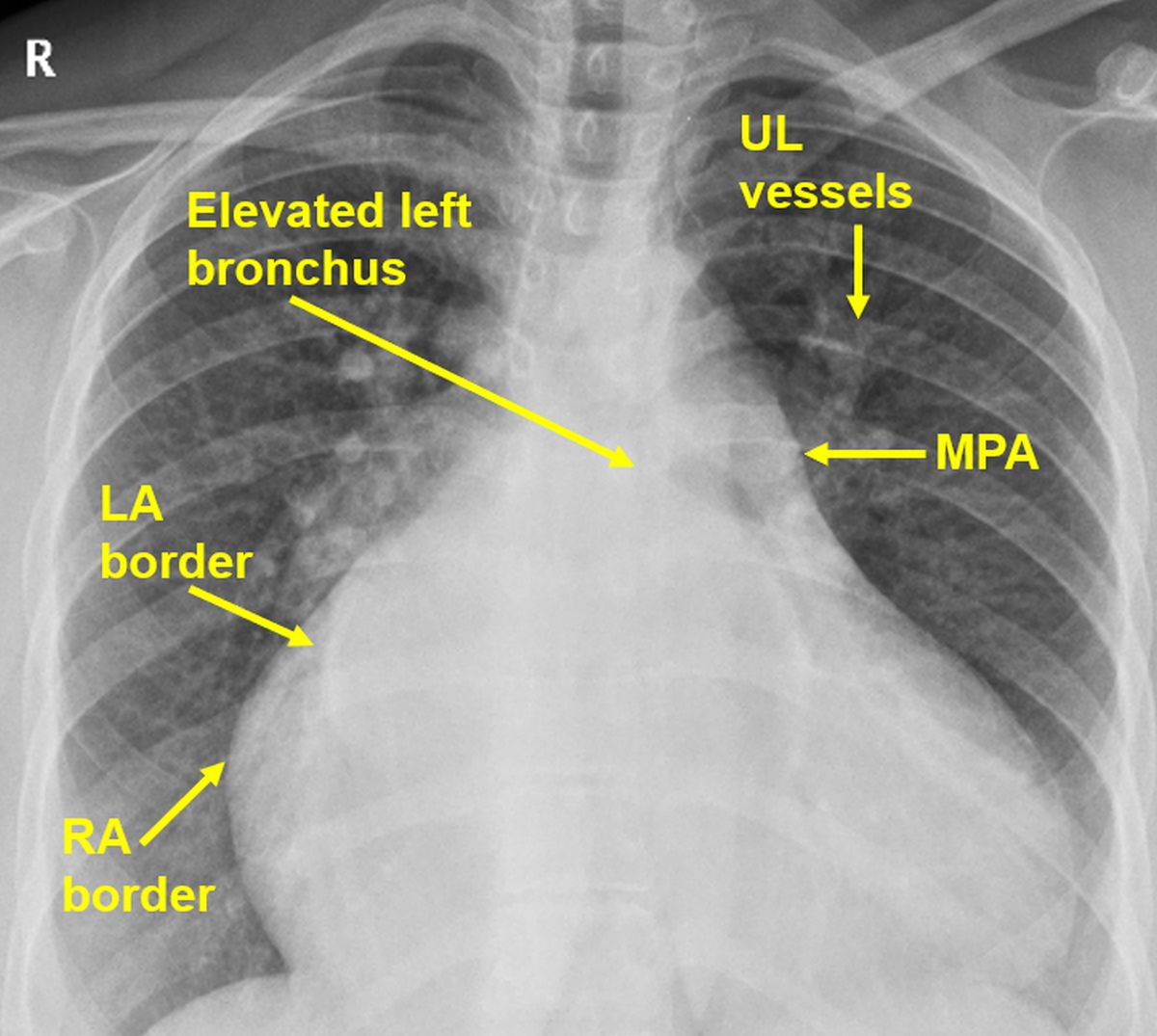 Biatrial enlargement on CXR causing cardiomegaly with a right ventricular pattern of apex (lifted up). Right atrial enlargement is evidenced by shift of the right cardiac border grossly to the right side. Left atrial enlargement is seen as a double contour within the right atrial shadow (shadow within shadow). Main pulmonary artery shadow is prominent on the left upper cardiac border. Right hilum is prominent due to enlargement of right pulmonary artery. Upper lobe vessels are prominent (inverted mustache sign, stag’s antler sign, cephalization). Antler sign indicates pulmonary venous hypertension [1]. The cited article gives the picture of a stag with antler superimposed on the chest X-ray for comparison! (Free full text). The article also lists a non cardiac cause for antler sign (lung torsion).
Biatrial enlargement on CXR causing cardiomegaly with a right ventricular pattern of apex (lifted up). Right atrial enlargement is evidenced by shift of the right cardiac border grossly to the right side. Left atrial enlargement is seen as a double contour within the right atrial shadow (shadow within shadow). Main pulmonary artery shadow is prominent on the left upper cardiac border. Right hilum is prominent due to enlargement of right pulmonary artery. Upper lobe vessels are prominent (inverted mustache sign, stag’s antler sign, cephalization). Antler sign indicates pulmonary venous hypertension [1]. The cited article gives the picture of a stag with antler superimposed on the chest X-ray for comparison! (Free full text). The article also lists a non cardiac cause for antler sign (lung torsion).
It is called cephalization because in normal pulmonary vasculature, lower lobe vessels are more prominent than upper lobe vessels. In pulmonary venous hypertension, there is redistribution of pulmonary blood flow towards the upper lobes, making upper lobe vessels more prominent.
Another manifestation of left atrial enlargement is elevation of left bronchus seen as the air bronchogram on CXR. The upturned apex is suggestive of right ventricular hypertrophy secondary to pulmonary arterial hypertension.
A sign which is expected, but missing, is the third mogul sign or prominent left atrial appendage below the main pulmonary artery. This can occur if the left atrial appendage had been removed earlier during a closed mitral valvotomy.
Left atrial appendage is a common site for thrombus in mitral stenosis and hence used to be removed during closed mitral valvotomy. The surgical procedure is seldom done now because balloon mitral valvotomy is the procedure of choice for symptomatic mitral stenosis.
Summarizing the findings, there is evidence of biatrial enlargement, pulmonary venous and arterial hypertension, and right ventricular hypertension. Together, these findings can occur in severe mitral stenosis. Down and out left ventricular type of apex would have been there if there was associated severe mitral regurgitation.
Any other cause of long standing left ventricular inflow obstruction like left ventricular endomyocardial fibrosis can also cause a similar picture. Only echocardiography will reveal the final diagnosis. Associated tricuspid regurgitation secondary to severe pulmonary hypertension is likely in view of right atrial enlargement.
Updated on 16 Jan 2021
Reference
- Han J, Xiang H, Ridley WE, Ridley LJ. Antler sign: Pulmonary venous hypertension. J Med Imaging Radiat Oncol. 2018 Oct;62 Suppl 1:13.
Related Posts

About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal