



Neither is universally “better” for a baseline diagnosis, as both carry Class I guideline recommendations for diagnosing heart failure and establishing prognosis. However, in contemporary clinical practice, NT-proBNP is generally preferred primarily due to its compatibility with current guideline-directed medical therapies and its distinct pharmacokinetic advantages.
Here is the clinical breakdown of why the shift toward NT-proBNP has occurred, along with the caveats where BNP still holds value.
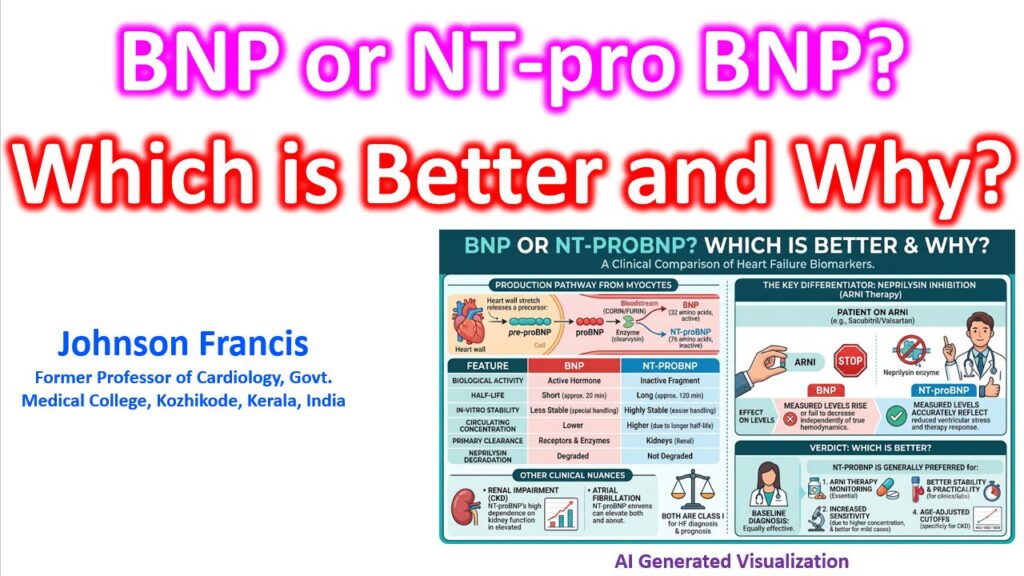
1. The ARNI (Sacubitril/Valsartan) Factor
This is the most significant clinical differentiator today.
- BNP is a direct substrate for neprilysin. When a patient is on an ARNI (Angiotensin Receptor-Neprilysin Inhibitor), neprilysin inhibition blocks the degradation of BNP. This causes measured BNP levels to rise—or fail to decrease—independently of the patient’s actual hemodynamic status.
- NT-proBNP is an inactive fragment that is not degraded by neprilysin; it is cleared passively. Therefore, NT-proBNP accurately reflects the true reduction in ventricular wall stress and improved hemodynamics when a patient responds to ARNI therapy. Current guidelines specifically recommend NT-proBNP over BNP for monitoring patients on an ARNI.
2. Half-Life and Diagnostic Sensitivity
When the cardiomyocyte is stretched, it secretes proBNP, which is cleaved by corin into equimolar amounts of BNP and NT-proBNP.
- BNP is the biologically active hormone with a short half-life of roughly 20 minutes.
- NT-proBNP is biologically inactive and has a half-life of roughly 120 minutes.
Because of this slower clearance, NT-proBNP circulates in much higher concentrations (roughly a 6:1 ratio in HFrEF, though this varies by atrial fibrillation status and renal function). This higher circulating concentration makes NT-proBNP a more sensitive marker for detecting earlier, milder forms of heart failure where BNP might still hover near normal limits.
3. In-Vitro Stability
From a laboratory and logistical standpoint, NT-proBNP is significantly more robust. BNP degrades rapidly at room temperature via contact activation of the coagulation system, requiring plastic tubes and rapid processing (or chilling) within 4 to 6 hours. NT-proBNP remains stable for several days at room temperature, making it far more practical for outpatient clinics where samples must be transported to a central lab.
Where BNP Still Holds Value (The Caveats)
While NT-proBNP is the standard for long-term monitoring, its strict reliance on renal clearance requires clinical nuance:
- Renal Impairment: Because NT-proBNP is strictly renally cleared, its levels are disproportionately elevated in patients with severe CKD compared to BNP (which enjoys dual clearance via neprilysin/neutral endopeptidases and NPR-C receptors). This is why NT-proBNP requires strict age-adjusted cutoffs to avoid false positives.
- Acute Hemodynamic Shifts: In a critical care or ICU setting, BNP’s rapid 20-minute half-life allows it to reflect acute, hour-to-hour hemodynamic changes faster than NT-proBNP, though practically this rarely dictates the choice of assay over NT-proBNP.
Ultimately, while both are excellent diagnostic tools, the evolution of GDMT makes NT-proBNP the more reliable, future-proof biomarker for the longitudinal, lifetime management of heart failure patients.