



Cardiac Autonomic Neuropathy (CAN) is a serious but often underdiagnosed complication of diabetes (and occasionally other metabolic disorders) where the autonomic nervous system, which controls involuntary heart and blood vessel functions, becomes damaged. It essentially disrupts the “autopilot” of the cardiovascular system, leading to issues with heart rate control and blood pressure regulation.
## Clinical Manifestations
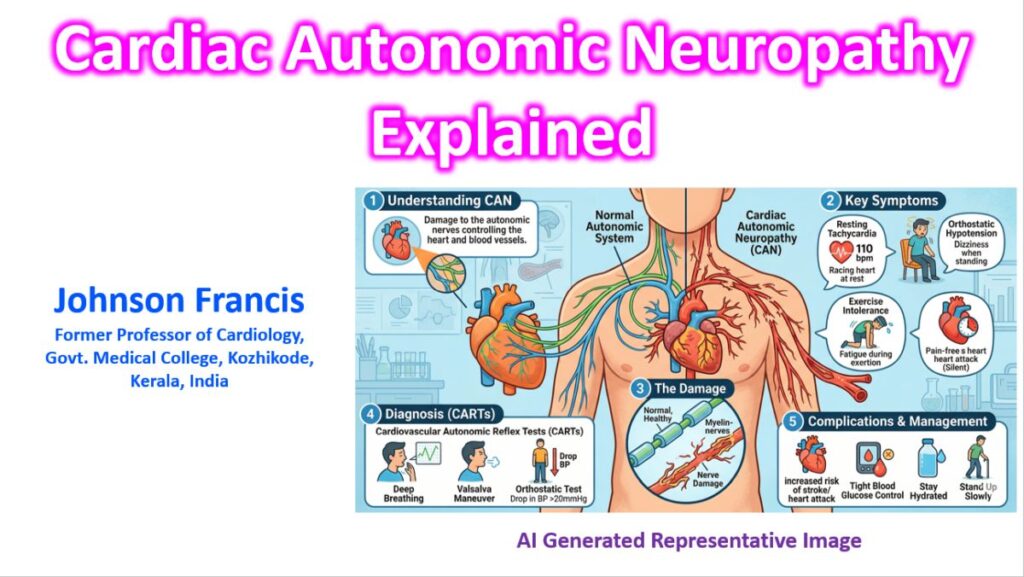
The symptoms can range from subtle to life-threatening. Key indicators include:
- Resting Tachycardia: A consistently high heart rate even during sleep or rest, caused by a loss of vagal (parasympathetic) tone.
- Orthostatic Hypotension: A significant drop in blood pressure when standing up, leading to dizziness, lightheadedness, or syncope.
- Exercise Intolerance: The heart fails to increase its rate appropriately in response to physical exertion (chronotropic incompetence).
- Silent Myocardial Ischemia: This is perhaps the most dangerous aspect; the nerves that transmit “chest pain” are damaged, meaning a patient might have a myocardial infarction without experiencing typical angina.
- Perioperative Instability: Increased risk of severe blood pressure swings or arrhythmias during general anesthesia.
## Risk Factors
Established risk factors for cardiac autonomic neuropathy are:
Glycemic control in Type 1 diabetes mellitus
Hypertension, dyslipidaemia, obesity, and glycaemic control in type 2 diabetes
## Diagnosis and Testing
Diagnosis typically involves Cardiovascular Autonomic Reflex Tests (CARTs), which are considered the gold standard:
| Test | Description | Abnormal Response |
| Valsalva Maneuver | Patient exhales against resistance. | Lack of expected heart rate slowing/speeding. |
| Heart Rate Variability (HRV) | Measuring R-R intervals during deep breathing. | Reduced variation (flattened rhythm). |
| Orthostatic Challenge | Moving from lying to standing. | SBP drop >20 mmHg or DBP drop >10 mmHg. |
| Test | Primary Measure | Clinical Significance |
| Deep Breathing | E:I Ratio | Assessment of vagal (parasympathetic) tone; often the first to become abnormal . |
| Valsalva Maneuver | Valsalva Ratio (Longest RR at rebound/Shortest at peak strain) | Tests both sympathetic and parasympathetic reflex arcs . |
| 30:15 Ratio (Peak HR at 15th beat and Least at 30th beat) | Postural R-R Change (Longest RR at beat 30/shortest RR at beat 15) | Measures the immediate heart rate response to standing . |
## Criteria for diagnosis and staging
- One abnormal cardiovagal test result identifies possible or early CAN
- At least two abnormal cardiovagal test results are required for definite or confirmed CAN
- The presence of orthostatic hypotension in addition to abnormal heart rate test results identifies severe or advanced CAN.
## Management Strategies
While the nerve damage itself is difficult to reverse, management focuses on symptom control and risk reduction:
-
- Glycemic Control: Intensive blood sugar management is the only proven way to slow the progression of CAN, especially in Type 1 diabetes.
-
- Lifestyle Modifications: For orthostatic hypotension, patients are often advised to increase salt/water intake, wear compression stockings, and move slowly when rising.
-
- Pharmacotherapy:
-
- Midodrine or Fludrocortisone for severe orthostatic hypotension.
-
- Beta-blockers (cautiously) for resting tachycardia.
-
- ACE inhibitors to provide cardioprotection.
-
- Pharmacotherapy:
-
- Screening: Annual screening for CAN is recommended for Type 2 diabetics at diagnosis and Type 1 diabetics five years after diagnosis.
Note: Because CAN is a strong predictor of cardiovascular mortality, patients with confirmed neuropathy require aggressive management of all other risk factors, including cholesterol and blood pressure.