



Cardiorenal Syndrome (CRS) describes the complex, bidirectional pathological interaction between the heart and the kidneys. In this relationship, dysfunction in one organ frequently initiates or exacerbates dysfunction in the other through shared hemodynamic, neurohormonal, and inflammatory pathways. The classification system developed by Ronco et al. (2008) is the gold standard for clinical categorization:
The Five Types of Cardiorenal Syndrome
| Type | Name | Primary Event | Resulting Action |
| Type 1 | Acute Cardiorenal | Acute Heart Failure (e.g., ADHF, Cardiogenic Shock) | Leads to Acute Kidney Injury (AKI) |
| Type 2 | Chronic Cardiorenal | Chronic Heart Failure | Leads to Chronic Kidney Disease (CKD) |
| Type 3 | Acute Renocardiac | Acute Kidney Injury (e.g., Glomerulonephritis, Ischemia) | Leads to Acute Cardiac Dysfunction (Arrhythmia, HF) |
| Type 4 | Chronic Renocardiac | Primary CKD | Leads to Cardiac hypertrophy, fibrosis, or CAD |
| Type 5 | Secondary | Systemic condition (e.g., Sepsis, Diabetes, Amyloidosis) | Leads to Simultaneous Heart & Kidney failure |
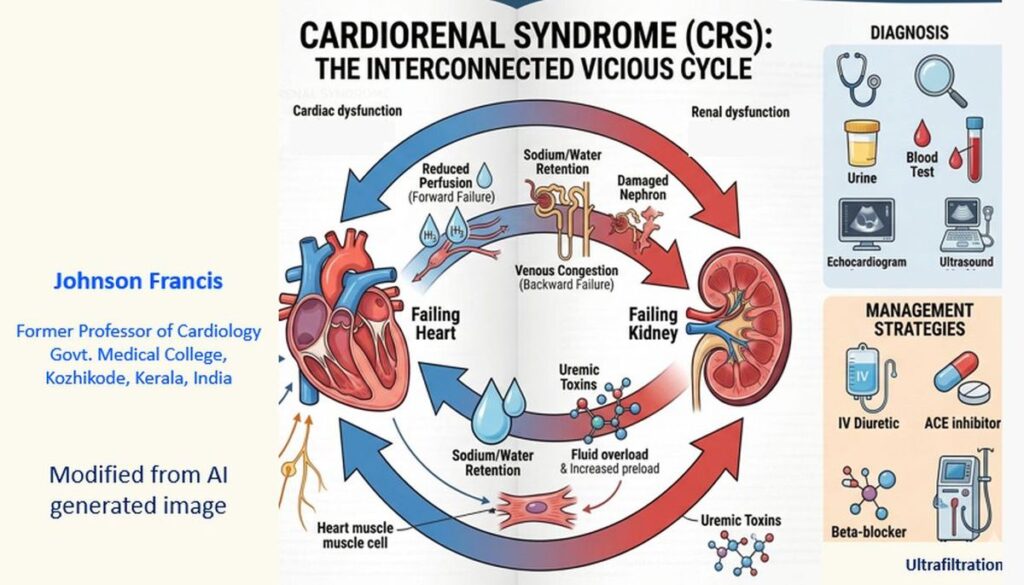
Pathophysiology: Why do they fail together?
The “vicious cycle” of CRS is driven by several key mechanisms:
- Hemodynamics: Reduced cardiac output leads to decreased renal perfusion. Conversely, high central venous pressure (venous congestion) increases renal interstitial pressure, reducing the glomerular filtration rate (GFR).
- RAAS Activation: Both heart and kidney failure trigger the Renin-Angiotensin-Aldosterone System, causing sodium/water retention and systemic vasoconstriction, which increases the workload on the heart.
- Sympathetic Nervous System (SNS): Chronic overactivity leads to further renal vasoconstriction and cardiac remodeling.
- Inflammation & Oxidative Stress: Shared cytokines (like TNF alpha and IL-6) promote fibrosis in both tissues.
Clinical Challenges
- Diuretic Resistance: As renal function declines, the kidneys become less responsive to loop diuretics, making fluid management in heart failure exceptionally difficult.
- Creatinine “Bumps”: During treatment for acute heart failure, serum creatinine often rises as fluid is removed. Deciding whether this is “permissive” AKI (treatment strategy to benefit long-term cardiovascular and kidney risk) or true renal damage is a common clinical dilemma.
Management Strategies
- Decongestion: Loop diuretics are first-line, often supplemented by thiazides or metolazone to overcome resistance.
- GDMT: Use of ACE inhibitors, ARBs, or ARNIs (Sacubitril/Valsartan), though these require careful monitoring of K+ and GFR. Combination of ACE inhibitors with ARB is discouraged. All these are mainly for chronic cardiorenal syndrome.
- SGLT2 Inhibitors: These have emerged as a “bridge” therapy, providing both cardioprotective and renoprotective benefits.
- Ultrafiltration: Reserved for patients with refractory fluid overload who do not respond to pharmacological therapy.