



Carotid artery stenting (CAS) has evolved significantly over the past two decades, transitioning from an alternative for high-surgical-risk patients to a mainstream revascularization strategy with a highly nuanced patient selection process.
Indications and Patient Selection
The decision between CAS, Carotid Endarterectomy (CEA), and Guideline-Directed Medical Therapy (GDMT) alone hinges on symptom status, anatomical factors, and patient comorbidities.
- Symptomatic Patients: CAS is typically a Class IIa recommendation for patients with recent TIA or ischemic stroke and 50% to 99% stenosis who have a high surgical risk for CEA (e.g., radiation-induced stenosis, previous neck surgery, contralateral vocal cord paralysis, or severe cardiopulmonary comorbidities).
- Asymptomatic Patients: The threshold for intervention is much higher, and GDMT (high-intensity statins, targeted antiplatelet therapy, strict BP control) remains the cornerstone. CAS or CEA may be considered in highly selected asymptomatic patients with >70% stenosis if the risk of periprocedural stroke or death is strictly <3%.
- Anatomical Unsuitability for CAS: Severe tortuosity of the aortic arch (Type III arch), heavy concentric calcification, or highly friable, thrombus-laden plaques strongly favor CEA over transfemoral CAS.
CAS vs. CEA: The Clinical Evidence
The debate between CAS and CEA is anchored by several landmark randomized controlled trials, with the CREST (Carotid Revascularization Endarterectomy vs. Stenting Trial) data driving much of the current practice.
| Trial / Factor | Key Findings |
| CREST-1 | Showed equivalent long-term outcomes for the primary composite endpoint of stroke, MI, and death. However, periprocedural differences were clear: CAS had a higher risk of minor stroke, while CEA had a higher risk of myocardial infarction. |
| SAPPHIRE | Demonstrated that CAS was non-inferior (and arguably superior in the short term) to CEA in patients specifically identified as high-risk for open surgery. |
| Age | Subgroup analyses consistently show that CEA is generally safer for patients >70 years old (increased arch tortuosity and calcification raise catheter-related embolic risk during CAS), whereas CAS performs equally well or better in younger cohorts. |
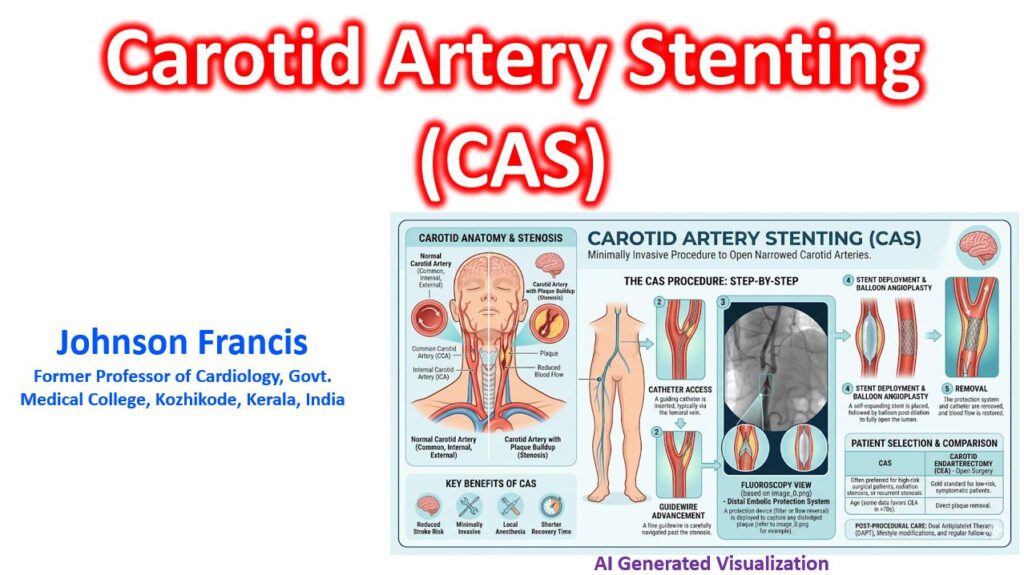
Procedural Nuances & Embolic Protection
The historical vulnerability of CAS has been atheroembolic stroke during lesion crossing and stent deployment. The mandatory use of Embolic Protection Devices (EPDs) has drastically reduced these periprocedural events. Currently, there are two primary approaches:
- Distal Filters: The most common EPD. A micro-filter is navigated past the lesion and deployed in the distal Internal Carotid Artery (ICA) to catch debris before balloon angioplasty and stent deployment.
- Proximal Protection: Devices involve inflating balloons in the Common Carotid Artery (CCA) and External Carotid Artery (ECA) to arrest or reverse flow. This prevents distal embolization without the operator needing to cross the lesion unprotected first.
The Shift Toward TCAR
Transcarotid Artery Revascularization (TCAR) has emerged as a disruptive hybrid approach. By accessing the CCA directly through a small supraclavicular incision, TCAR completely avoids navigating a catheter through the aortic arch—eliminating a major source of embolic strokes in elderly patients.
It utilizes a robust flow-reversal circuit (shunting blood from the carotid to the femoral vein) prior to crossing the carotid lesion. While the field awaits definitive RCTs comparing TCAR directly to CEA, current registry data suggests TCAR achieves periprocedural stroke rates rivaling open endarterectomy, while maintaining the minimally invasive benefits of stenting.
Comparisons to CEA: In an analysis of the Vascular Quality Initiative (VQI) registry comparing over 1,100 TCAR procedures to over 10,000 Carotid Endarterectomy (CEA) procedures, researchers found that despite TCAR patients possessing substantially higher medical risk, the in-hospital stroke and death rates were similar between the two groups.
Foundational Clinical Trials for carotid artery stenting (CAS)
- The CREST Trial (2010): The Carotid Revascularization Endarterectomy versus Stenting Trial is a landmark study that compared CAS to carotid endarterectomy (CEA). It established that there was no significant difference in the composite primary outcome of stroke, myocardial infarction, or death between the two procedures over a median follow-up of 2.5 years. There was a higher risk of stroke with stenting and a higher risk of myocardial infarction with endarterectomy in the periprocedural period.
- The SAPPHIRE Trial (2004): This trial evaluated patients with severe carotid-artery stenosis and coexisting conditions that placed them at a high risk for surgical complications. It concluded that CAS utilizing an emboli-protection device was not inferior to open endarterectomy for this high-risk population.
- The ACT 1 Trial (2016): Focused specifically on asymptomatic patients who were not at high risk for standard surgical complications. The trial demonstrated that CAS was noninferior to CEA with regard to the primary composite endpoint of death and stroke at 1 year.
Clinical Guidelines
- AHA/ASA Secondary Stroke Prevention Guidelines (2021): The American Heart Association and American Stroke Association provide definitive clinical practice guidelines for preventing recurrent strokes. This document outlines optimal medical therapy, indications for intervention in extracranial carotid artery disease, and specific patient selection criteria for stenting versus endarterectomy.
- ESVS Clinical Practice Guidelines (2023): The European Society for Vascular Surgery published updated and highly comprehensive guidelines covering the medical, endovascular, and surgical management of atherosclerotic carotid and vertebral artery disease.