



Coarctoplasty (also known as Balloon Angioplasty for Coarctation of the Aorta) is a minimally invasive procedure used to treat a coarctation of aorta. Earlier the term was used for surgical coarctoplasty. But now it is being increasingly used for balloon dilatation of coarctation, usually followed by stenting. COAST and COAST II Trials had five year data published recently.
Procedure
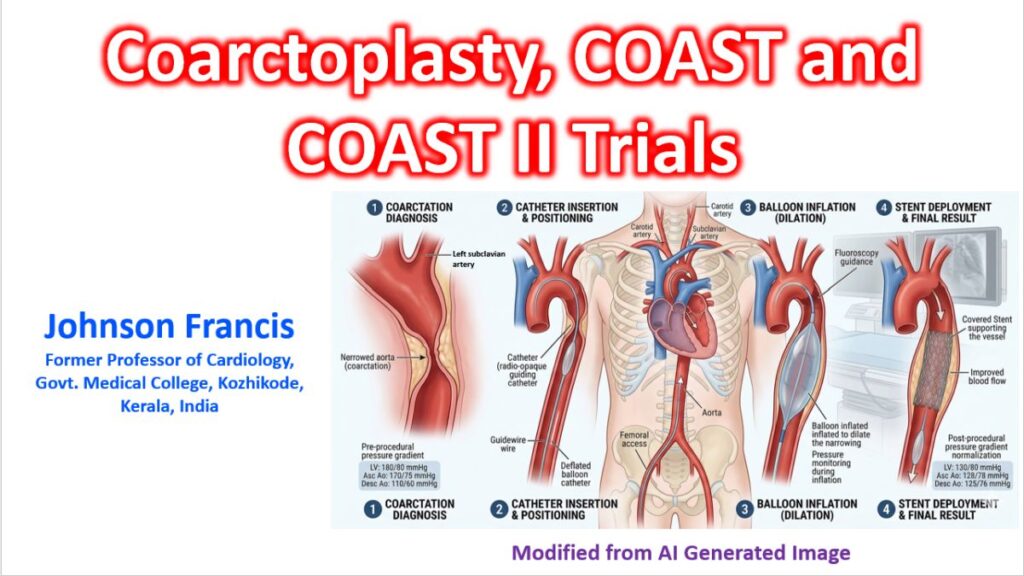
Coarctoplasty is performed in a cardiac catheterization lab.
- Percutaneous catheter access is through the femoral artery.
- Using fluoroscopy catheter is moved to the site of coarctation in the descending aorta.
- A balloon at the tip of the catheter is inflated, stretching the narrowed segment of the aorta to improve blood flow.
- In many cases (especially in adolescents and adults), a stent is expanded and left in place to keep the aorta from rebounding.
Indications
Coarctoplasty is primarily used in three scenarios:
- Native Coarctation: Treating the narrowing for the first time, often preferred in older children and adults.
- Recurrent Coarctation: Treating a narrowing that has returned after a previous surgical repair (re-coarctation).
- Critically ill neonates: Sometimes used as a “bridge” to stabilize a sick infant before they are strong enough for definitive surgery.
Key Risks and Considerations
While generally safe, the procedure carries specific risks:
- Aneurysm Formation: The stretching of the vessel wall can sometimes weaken it, leading to aneurysm formation years later.
- Restenosis: The area may narrow again as the child grows or due to scar tissue.
- Vessel Injury: Small risk of tearing the aorta/dissection or damaging the access artery in the groin. A recent report of 274 children noted major vascular access complications in 18 patients (6.6%) and acute limb ischemia in 8 (2.9%).
Lifelong follow-up is mandatory after coarctoplasty. Even after a “successful” procedure, patients remain at a higher risk for hypertension later in life.
COAST COAST II trials
5 years of postimplant follow-up in patients enrolled into the COAST (Coarctation of the Aorta Stent Trial) and the COAST II trial (Covered Cheatham-Platinum Stents for Prevention or Treatment of Aortic Wall Injury Associated With Coarctation of the Aorta), evaluating the bare and Covered Cheatham-Platinum Stents for the treatment of coarctation of the aorta and associated aortic wall injury have been reported recently. They were multi-center studies enrolling 248 patients, 121 in COAST and 127 patients in COAST II. Late follow-up data was compared with immediate (1 month) and early (1 year) data. COAST II had used covered stents. The report concluded that coarctation stenting is effective at maintaining relief of obstruction up to 5 years post implant and reduction in number of patients requiring antihypertensive medication. But there was an increase in stent fracture and reinterventions between medium and long-term follow up. There was some protection against the development of stent fracture with covered stents, but did not provide complete protection from late aneurysm formation.