



Congenital anomalies of the aortic arch arise from the abnormal regression or persistence of the embryonic branchial arches (specifically the fourth arch and the dorsal aortae). While many of these variations are benign, incidental findings, others cause significant structural and hemodynamic compromise. Here is a breakdown of the most clinically important arch anomalies and their practical significance.
1. Double Aortic Arch (DAA)
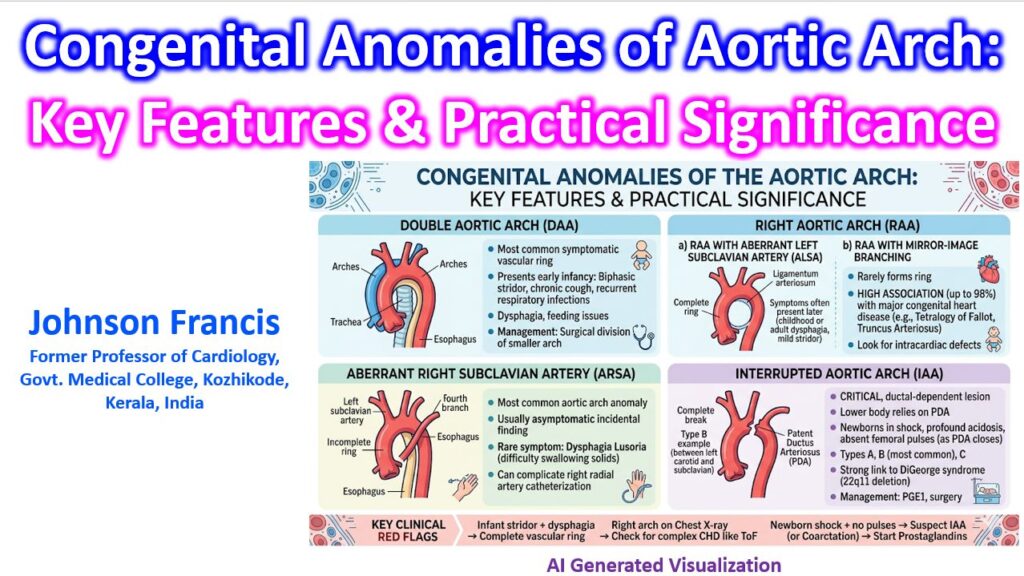
A double aortic arch occurs when both the right and left embryonic arches persist, creating a complete “vascular ring” that encircles the trachea and the esophagus.
- Anatomy: The ascending aorta splits into two arches that pass on either side of the trachea and esophagus before rejoining to form the descending aorta. Usually, the right arch is dominant (larger and higher).
- Practical Significance: This is the most common cause of a symptomatic vascular ring. It typically presents early in infancy.
- Respiratory: Tracheal compression leads to biphasic stridor, chronic cough, wheezing, and recurrent respiratory infections. Symptoms often worsen during feeding or crying.
- Gastrointestinal: Esophageal compression causes dysphagia or vomiting.
- Management: Surgical division of the smaller arch (usually the left) is required to relieve the compression.
2. Right Aortic Arch (RAA)
A right aortic arch occurs when the left embryonic arch regresses and the right arch persists. Its clinical significance depends entirely on its branching pattern and whether a vascular ring is formed.
RAA with Aberrant Left Subclavian Artery (ALSA)
- Anatomy: The arch crosses to the right of the trachea. The left subclavian artery arises as the last branch and crosses behind the esophagus to reach the left arm.
- Practical Significance: This forms a complete vascular ring because the left ligamentum arteriosum connects the ALSA (or the descending aorta) to the left pulmonary artery, trapping the airway and esophagus. However, it is often looser than a DAA, so symptoms (if any) may present later in childhood or adulthood as dysphagia or mild stridor.
RAA with Mirror-Image Branching
- Anatomy: The arch is on the right, and the branches arise in reverse order of a normal left arch (Left brachiocephalic, right common carotid, right subclavian).
- Practical Significance: This rarely forms a vascular ring, so airway compression is not the issue. However, it has a very high association (up to 98%) with major congenital heart disease, most notably Tetralogy of Fallot and Truncus Arteriosus. Finding this on an echocardiogram mandates a meticulous search for intracardiac defects.
3. Left Aortic Arch with Aberrant Right Subclavian Artery (ARSA)
This is the most common congenital anomaly of the aortic arch, occurring in roughly 1% to 2% of the general population.
- Anatomy: The right subclavian artery does not arise from the brachiocephalic trunk. Instead, it originates as the fourth (and last) branch of the aortic arch and courses behind the esophagus to reach the right arm.
- Practical Significance: It is an incomplete ring (no airway compression) and is asymptomatic in the vast majority of patients.
- Dysphagia Lusoria: In rare cases, the artery compresses the esophagus against the trachea, causing difficulty swallowing solid foods in adults.
- Procedural Impact: If performing a right radial artery catheterization, the guidewire may take an unexpected downward turn into the descending aorta rather than the ascending aorta, complicating access to the coronary arteries.
4. Interrupted Aortic Arch (IAA)
This is a critical, life-threatening anomaly where there is a complete anatomic and luminal discontinuity between the ascending and descending aorta.
- Anatomy: Classified based on where the interruption occurs:
- Type A: Distal to the left subclavian artery.
- Type B: Between the left common carotid and left subclavian (most common).
- Type C: Between the innominate artery and left common carotid (rarest).
- Practical Significance: This is a ductal-dependent lesion. The lower half of the body relies entirely on blood flow from the right ventricle across the patent ductus arteriosus (PDA).
- Presentation: Infants present with profound cardiogenic shock, absent femoral pulses, and severe metabolic acidosis immediately after birth as the PDA begins to close.
- Genetics: Type B is strongly associated with DiGeorge syndrome (22q11.2 microdeletion).
- Management: Immediate infusion of Prostaglandin E1 (PGE1) to maintain ductal patency is lifesaving, followed by complex surgical reconstruction.
Summary of Clinical Red Flags
When evaluating a patient with a suspected arch anomaly, keep these practical rules in mind:
- Stridor + Dysphagia in an infant: Suspect a complete vascular ring, primarily a Double Aortic Arch.
- Right Aortic Arch on Chest X-Ray: If it has mirror-image branching, look for Tetralogy of Fallot.
- Shock in a newborn + absent lower pulses: Suspect an Interrupted Aortic Arch (or severe coarctation) and start Prostaglandins immediately.