



Congenital coronary artery anomalies (CCAAs) are a diverse group of malformations involving the origin, course, or structure of the coronary arteries. While most are benign and discovered incidentally during angiography or CT, certain subtypes carry a high risk of myocardial ischemia, heart failure, or sudden cardiac death (SCD).
## Clinical Classification
CCAAs are generally categorized based on their functional significance:
1. Hemodynamically Significant (High Risk)
These anomalies can compromise myocardial perfusion, especially during exertion.
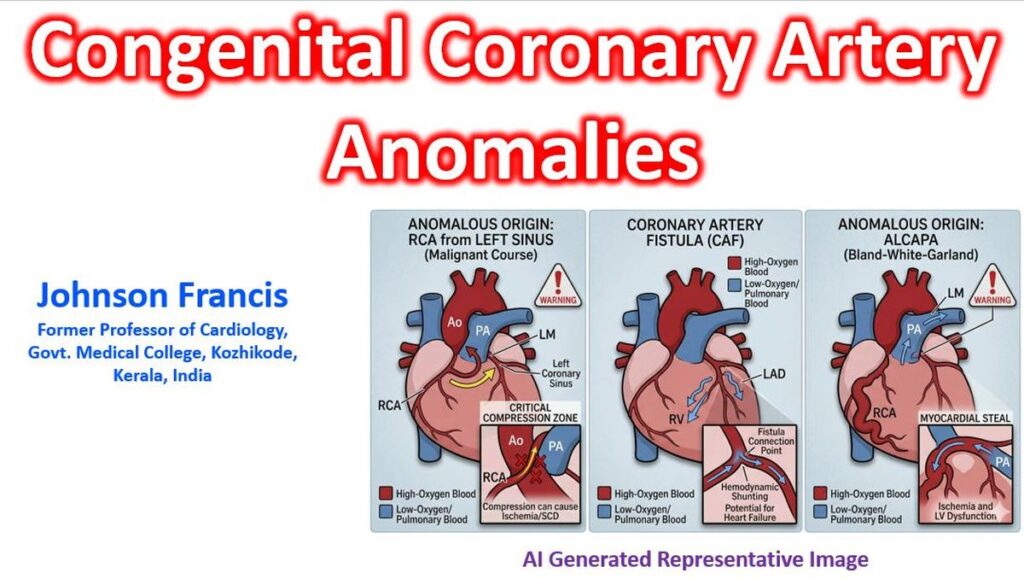
- Anomalous Origin from the Pulmonary Artery (ALCAPA): Most commonly the Left Main (Bland-White-Garland syndrome). It leads to a “steal” phenomenon where blood flows from the coronary system into the low-pressure pulmonary artery.
- Interarterial Course (Malignant Course): An artery (often the Right Coronary Artery) originates from the opposite sinus and passes between the aorta and the pulmonary artery. Compression during exercise can lead to sudden death.
- Congenital Atresia: Complete absence of a coronary ostium, usually the Left Main.
- Coronary Artery Fistulae: Abnormal communication between a coronary artery and a cardiac chamber or major vessel (e.g., the Right Ventricle or Pulmonary Artery).
2. Hemodynamically Insignificant (Benign)
- High Takeoff: Origin of the ostium >1 cm above the sinotubular junction.
- Duplicate Vessels: Such as a double Left Anterior Descending (LAD) artery.
- Circumflex (LCx) from the Right Sinus: This is the most common origin anomaly and is typically asymptomatic unless it takes a retroaortic course that complicates valve surgery.
## Diagnostic Modalities
Given the complex 3D anatomy, traditional invasive angiography is often supplemented by advanced imaging:
- Coronary CT Angiography (CCTA): The gold standard. It provides superior spatial resolution to define the “malignant” interarterial course.
- Cardiac MRI (CMR): Excellent for pediatric patients to avoid radiation and for assessing myocardial viability/ischemia.
- Transthoracic Echocardiography (TTE): Primary screening tool in infants (especially for ALCAPA), though limited in adults by acoustic windows.
## Key Clinical Consideration: Sudden Cardiac Death (SCD)
In young athletes, anomalous coronary origins are the second most common cause of SCD after Hypertrophic Cardiomyopathy (HCM). The “malignant” course is particularly dangerous because exercise-induced expansion of the aorta and pulmonary artery can “pinch” the anomalous vessel, leading to fatal arrhythmias.
## Common CHDs Associated with CCAAs
While Congenital Coronary Artery Anomalies (CCAAs) can occur in isolation, they are frequently associated with various other structural congenital heart diseases (CHDs). In the context of complex CHD, identifying coronary anomalies is essential, as abnormal coronary anatomy often dictates surgical approaches and complicates myocardial protection during repair. Certain types of CHD have a high prevalence of associated coronary anomalies. The specific anomaly often varies by the type of heart defect. Coding of coronary arteries according to the Leiden convention: 1, sinus 1; 2, sinus 2; L, left anterior descending; Cx, left circumflex; R, right coronary artery. e.g. 1L‐2CxR
1. D-Transposition of the Great Arteries (d-TGA)
d-TGA is almost inherently associated with variations in coronary anatomy because the coronary arteries must arise from the posterior great vessel (which is the aorta in this condition).
- Specific Anomalies: The single most common anomaly in d-TGA is the Left Circumflex (LCx) artery arising from the Right Coronary Artery (RCA) (1L‐2CxR). A single coronary artery arising from the left sinus is also common.
- Clinical Impact: The primary surgical treatment, the Arterial Switch Operation, requires the transfer of the coronary buttons to the neoaorta. These complex coronary patterns make the operation significantly more challenging and increase the risk of procedural myocardial ischemia.
2. Tetralogy of Fallot (ToF)
Coronary artery anomalies occur in roughly 5–10% of cases of classic ToF.
- Specific Anomalies: The most common is the Left Anterior Descending (LAD) artery arising from the RCA or right sinus of Valsalva and crossing the right ventricular outflow tract (RVOT). Other variants include a dominant RCA or single coronary artery.
- Clinical Impact: A coronary artery crossing the RVOT is a major surgical contraindication for a large transannular patch (standard repair), as it runs the risk of transection during ventriculotomy. This scenario often requires an alternative repair strategy, such as placement of a right ventricle-to-pulmonary artery conduit to bypass the vessel.
3. Pulmonary Atresia with Intact Ventricular Septum (PA/IVS)
CCAAs, particularly coronary-sinusoid fistulae, are extremely prevalent in PA/IVS, affecting up to 30–50% of patients.
- Specific Anomalies:
- Coronary Sinusoid Fistulae: High pressure in the right ventricle forces blood through persistent sinusoids into the coronary circulation (RV-dependent coronary circulation).
- Coronary Stenosis or Atresia: Common in this patient subset.
- Clinical Impact: Decompressing the high-pressure right ventricle in PA/IVS can paradoxically cause fatal myocardial ischemia if the ventricular coronary fistulae and associated proximal stenoses mean the circulation relies on the high RV pressure for perfusion. Surgical strategies must protect this delicate circulation.
4. Other Conditions
- Truncus Arteriosus: Associated with single coronary artery patterns and anomalies in ostial location, which can complicate the placement of a surgical conduit.
- Single Ventricle Physiology (e.g., Hypoplastic Left Heart Syndrome): While not universally present, abnormal coronary connections can complicate the complex staged reconstruction (Norwood, Glenn, Fontan procedures) by creating competing runoff or limiting venous return.
- Supravalvular Aortic Stenosis (e.g., Williams Syndrome): Associated with unique coronary issues where the arteries are exposed to high systolic pressure, leading to tortuosity, dilation, and premature atherosclerosis, and coronary ostial stenosis.
## Summary of Key Associations
| Congenital Heart Disease | Associated Coronary Anomaly (Typical) | Critical Impact on Management |
| d-TGA | LCx from RCA; Single Coronary Artery (SCA) from left | Complicates coronary artery transfer during Arterial Switch Operation (ASO). |
| Tetralogy of Fallot | LAD from RCA (crosses RVOT) | Precludes a large transannular patch; requires alternative conduit repair. |
| PA/IVS | RV-to-Coronary Fistulae; Stenosis/Atresia | Decompressing the RV may cause fatal ischemia (RV-dependent coronary circulation). |
| Truncus Arteriosus | High/abnormal ostia; SCA patterns | Influences surgical conduit choice and placement. |
## Diagnostic and Surgical Considerations
- Preoperative Imaging: In complex CHD cases, advanced non-invasive imaging, particularly Coronary CT Angiography (CCTA), is often vital to accurately define the coronary anatomy before repair. Cardiac MRI is also used, though CT provides better resolution.
- “Malignant” Implications: While the interarterial course is the primary “malignant” anomaly in isolated hearts, in complex CHD, the definition of risk shifts to how an anomaly restricts surgical feasibility or poses unique risks to survival (e.g., the crossing artery in ToF or RV-dependence in PA/IVS).