



In survivors of sudden cardiac death (SCD), coronary artery disease (CAD) is the most common underlying etiology, identified in approximately 70% to 80% of cases. Consequently, coronary angiography and revascularization are central to the diagnostic and therapeutic pathway. Current guidelines emphasize that the timing and necessity of these interventions are heavily dictated by the presence of ST-segment elevation (STEMI) and hemodynamic stability.
Role of Coronary Angiography
Angiography serves both a diagnostic role (identifying the “culprit” lesion) and a prognostic role (assessing the extent of CAD).
Immediate Angiography (< 2 hours)
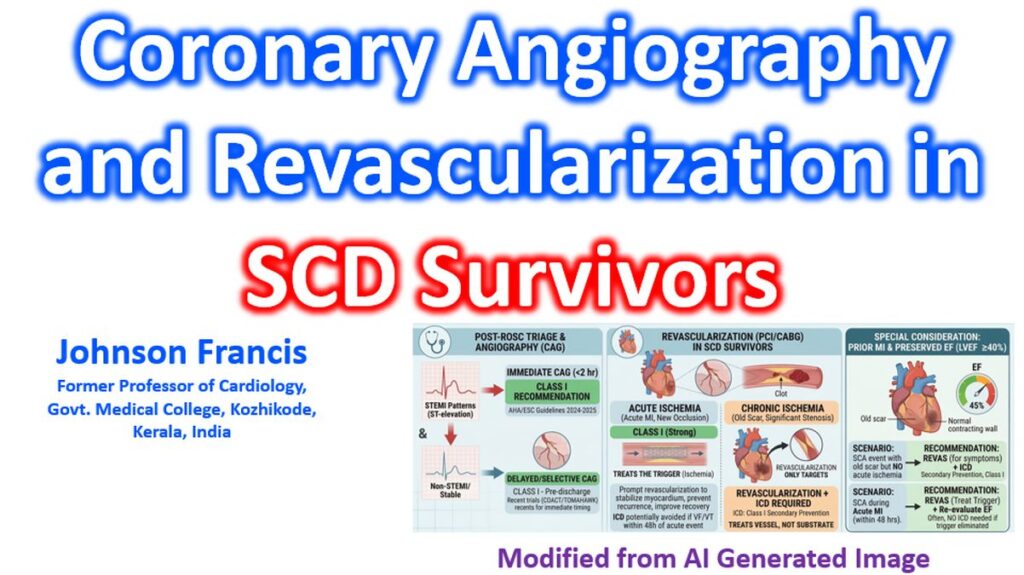
- STEMI on post-ROSC ECG: Immediate angiography is a Class I recommendation. The presence of ST-elevation is a strong predictor of an acute coronary occlusion.
- Hemodynamic Instability: Even without ST-elevation, patients in cardiogenic shock or with life-threatening arrhythmias (e.g., electrical storm) should undergo immediate invasive assessment.
Delayed or Selective Angiography
- Non-STEMI Patients: For stable survivors without ST-elevation, recent randomized trials (COACT, TOMAHAWK) have shown that immediate angiography does not improve survival or neurological outcomes compared to a delayed approach.
- Pre-Discharge Recommendation: Guidelines recommend coronary angiography before hospital discharge for all cardiac arrest survivors with a suspected cardiac etiology, particularly those with a shockable rhythm or unexplained LV dysfunction.
Role of Revascularization
Revascularization (PCI or CABG) aims to stabilize the myocardium, prevent recurrent arrhythmias, and preserve left ventricular (LV) function.
- Acute Benefit: In the setting of an acute coronary syndrome (ACS), prompt revascularization reduces the risk of re-infarction and improves post-resuscitation hemodynamics.
- Arrhythmia Suppression: Revascularization can eliminate the “trigger” (ischemia) for ventricular fibrillation (VF). However, it may not address the “substrate” (old scar/fibrosis), meaning an ICD is often still required for secondary prevention.
- LV Recovery: Successful reperfusion can reverse myocardial hibernation or stunning, potentially improving the ejection fraction (EF) over the following 3 months.
Key Considerations for the Clinical Team
| Scenario | Recommendation | Rationale |
| Post-ROSC STEMI | Emergency PCI | High probability of acute occlusion; time-sensitive survival benefit. |
| Post-ROSC NSTEMI (Stable) | Delayed Angiography | Allows for neurological assessment and stabilization; no benefit found for “emergency” timing. |
| Complex Multi-vessel CAD | Heart Team Discussion | To decide between PCI and CABG based on Syntax score and patient frailty. |
| Severe LV Dysfunction | Re-evaluate EF at 90 days | Revascularization may improve EF; ICD eligibility is usually reassessed after a waiting period. |
Limitations & Caveats
- Neurological Status: In comatose survivors, the decision to proceed with invasive intervention must be balanced against the perceived neurological prognosis, which is often difficult to determine in the first 72 hours.
- The “No-Reflow” Phenomenon: Post-cardiac arrest syndrome involves systemic inflammation and microvascular dysfunction, which can sometimes complicate the success of PCI.
In survivors of sudden cardiac death (SCD) who have a prior myocardial infarction (MI) but preserved or mildly reduced ejection fraction (LVEF ≥40%), the role of revascularization is primarily focused on eliminating ischemia as a trigger for recurrent ventricular arrhythmias (VA).
Revascularization for Secondary Prevention
The core principle is that if the SCD event was clearly “triggered” by an acute ischemic event (like a new MI), revascularization is the primary treatment. However, if the event was due to an old scar (substrate), the recommendation changes.
- Class I (Strong): Revascularization is recommended in survivors of SCD who have significant coronary artery stenosis and evidence of ongoing or acute ischemia that is suspected to have triggered the arrhythmia.
- Class I (Strong): In patients with a prior MI and preserved EF who present with hemodynamically unstable ventricular tachycardia (VT) or VF in the setting of an acute coronary syndrome (ACS), prompt revascularization is required.
ICD vs. Revascularization in Preserved EF
This is the “gray area” for many clinicians because most ICD trials (like MADIT-II or SCD-HeFT) focused on low EF (≤35%).
- Class I (Secondary Prevention): An ICD is recommended for survivors of SCD due to VF or hemodynamically unstable VT that is not due to a reversible cause (such as acute ischemia within 48 hours of an MI).
- Note: If the SCD occurred and you find an old scar with significant stenosis but no acute occlusion, revascularization alone is often considered insufficient; the ICD remains a Class I recommendation regardless of the EF.
- Class IIa (Moderate): In patients with a prior MI and preserved EF who have sustained monomorphic VT that is hemodynamically well-tolerated, catheter ablation or revascularization (if ischemia is present) is reasonable, often in conjunction with or as an alternative to an ICD.
Summary of Revascularization “Value”
| Clinical Scenario | Recommendation Class | Key Rationale |
| SCD + Acute MI (STEMI/NSTEMI) | Class I | Revascularization treats the acute “trigger.” |
| SCD + Chronic CAD (No acute ischemia) | Class I (for ICD) | Revascularization may be done, but does not replace the need for an ICD (substrate remains). |
| SCD + Coronary Vasospasm | Class IIa | ICD should be considered even if revascularization or medical therapy is performed. |
The “48-Hour” Rule
It is critical to distinguish if the SCD occurred within the first 48 hours of an acute MI. If revascularization is performed and the arrhythmia occurred during that acute phase, it is considered “reversible,” and an ICD is generally not indicated. If the arrhythmia occurs after the first 48 hours, even with preserved EF, the risk of recurrence is high enough to warrant an ICD.
Useful reference which includes a summary of COACT and TOMAHAWK trials: Coronary Revascularization and Out-of-hospital Cardiac Arrest: Past, Present and Future.
2023 ESC Guidelines for the management of acute coronary syndromes
2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure