


Managing coronary bifurcation lesions (CBLs) requires balancing side-branch (SB) protection, stent optimization, and long-term vessel patency. Because plaque or carina shifts during main vessel (MV) expansion can jeopardize the side branch, standardizing the approach based on lesion anatomy and fractal geometry is critical.
1. Core Architectural Principles & Risk Stratification
Fractal Geometry & Vessel Sizing
Sizing of the proximal main vessel (pMV), distal main vessel (dMV), and side branch (SB) must respect the fractal geometry of the bifurcation. Over-expanding the distal vessel or under-expanding the proximal vessel can induce flow disturbances, edge dissections, or acute stent malapposition. Sizing calculations should align with Finet’s Law:
DpMV = 0.678 x (DdMV + DSB)
Predictors of Side-Branch Compromise
True bifurcation lesions (Medina 1,1,1 or 1,0,1) with extensive ostial disease represent the highest risk. Pre-procedural intravascular imaging—specifically Optical Coherence Tomography (OCT)—identifies high-risk structural features. Plaque distribution located within the proximal main branch, prominent calcified plaque characteristics, and a narrow bifurcation/carina angle (≤ 80°) serve as significant independent predictors of acute SB ostial compromise during crossover stenting.
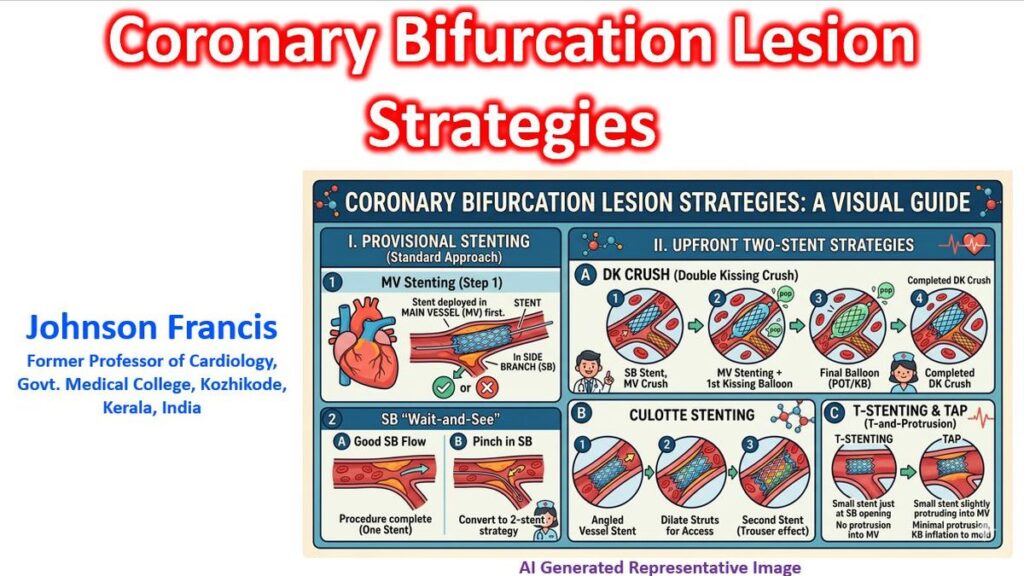
2. Stepwise Provisional Stenting (The Workhorse Strategy)
The European Bifurcation Club (EBC) recommends a stepwise provisional stenting (PS) strategy as the default approach for the vast majority of bifurcation lesions (Burzotta et al., 2024). Randomized trials (such as EBC TWO and EBC MAIN) confirm that minimizing the total metal burden results in comparable or superior long-term clinical outcomes compared to mandatory upfront two-stent approaches for SBs with short lesion lengths (< 10 mm) (Burzotta et al., 2024; Lassen et al., 2022).
[ Stepwise Provisional Pathway ]
│
(Wire both MV & SB)
│
(Stent MV across SB ostium)
│
┌──────────┴──────────┐
[ POT ] [ POT ]
(SB flow intact) (SB flow compromised)
│ │
(Leave Alone) (Rewire Distal Cell)
│
(KBI & Final POT)
│
(Bailout 2-Stent if needed)
The Technical Framework (The ABC Approach)
- Stage A — Dual Wiring: Both the MV and SB should be wired systematically. Utilizing the jailed wire technique (JWT) acts as a crucial safety net: it modifies the bifurcation angle favorably, keeps the ostium open, and provides a clear wire path for rescue balloons if the branch occludes. For highly threatened, tight ostia, a jailed balloon technique (JBT) can provide active physical protection against significant carina shift.
- Stage B — Lesion Preparation: In severely calcified or high-plaque-burden bifurcations, plaque modification via rotational/laser atherectomy or intravascular lithotripsy is required to guarantee subsequent stent expansion and wire re-crossability.
- Stage C — Stent Implantation & Optimization:
- Proximal Optimization Technique (POT): This step is mandatory. A short, non-compliant balloon sized 1:1 to the pMV reference is inflated just proximal to the carina. This corrects the inevitable proximal malapposition caused by sizing to the distal vessel and widens the stent struts directly over the SB ostium for easier rewiring.
- Distal Cell Rewiring: If the SB requires further dilation, pulling back and re-crossing the wire through the distal cell of the MV stent ensures optimal scaffolding and endothelial coverage of the SB ostium once ballooned.
- Conservative vs. Aggressive Branch Management: Data from the KISS (Keep Bifurcation Single Stenting Simple) trial confirms that if SB flow remains acceptable after MV stenting and POT, a conservative strategy (no routine SB intervention) is strictly noninferior to systematic SB ballooning regarding periprocedural MI, while significantly lowering radiation exposure, contrast use, and procedural complications like SB dissections.
3. Upfront Two-Stent Strategies
A planned, systematic dual-stent strategy is reserved for true bifurcation lesions with highly complex anatomy, a large and clinically significant SB (≥ 2.75 mm in diameter), or an extensive ostial disease length exceeding 10 mm.
| Strategy | Primary Indications | Key Procedural Nuance |
| Double Kissing Crush (DK-Crush) | Complex, true left main (LM) bifurcations; highly diseased SB ostium. | Requires a highly structured, 2-step sequential kissing balloon inflation (KBI) to completely clear metal layers and optimize ostial expansion. |
| Culotte / DK-Culotte | Similar vessel diameters between MV and SB; sharp bifurcation angles (< 70°). | Achieves near-perfect circumferential scaffolding, but results in a double layer of metal throughout the entire proximal MV segment. |
| T and Small Protrusion (TAP) | Shallow bifurcation angles; predominantly used as a bailout from provisional. | The SB stent is deployed with minimal protrusion into the MV, immediately followed by a final KBI to construct a precise “neo-carina”. |
4. Hybrid Techniques and Future Directions
- Hybrid DCB Strategy: To avoid the risk of late stent thrombosis and multi-layer restenosis associated with two-stent options, combining a contemporary DES in the MV with a Drug-Coated Balloon (DCB) in the SB is increasingly utilized. This strategy treats residual ostial disease effectively while respecting the “leaving nothing behind” philosophy for the branch vessel.
- Robotic-Assisted PCI: Robotic systems are introducing millimetric precision to complex bifurcation wiring, sub-millimeter POT balloon positioning, and controlled stent deployment at the carina core.
References
Albiero, R., Burzotta, F., Lassen, J. L., et al. (2022). Treatment of coronary bifurcation lesions, part I: implanting the first stent in the provisional pathway. The 16th expert consensus document of the European Bifurcation Club. EuroIntervention, 18(5), e362–e376.
An, X. et al. (2026) Challenges and optimization of percutaneous coronary interventions for coronary bifurcation lesions.
Burzotta, F., Louvard, Y., Lassen, J. F., et al. (2024). Percutaneous coronary intervention for bifurcation coronary lesions using optimised angiographic guidance: the 18th consensus document from the European Bifurcation Club. EuroIntervention, 20(15), e915–e926.
Chevalier, B. et al. (2026). Side branch additional treatment for coronary bifurcation lesion revascularization: Insights from the KISS randomized trial. JACC: Cardiovascular Interventions.
Dillen, D. M. M. et al. (2026). Hybrid drug-coated balloon strategy for coronary bifurcation lesions: a systematic review and meta-analysis. BMJ Open
Han, J et al. (2026). Association between plaque characteristics and side-branch compromise in left main bifurcation lesions after a single-stent crossover technique: insights from an optical coherence tomography study. Frontiers in Cardiovascular Medicine.
Lassen, J. L., Albiero, R., Johnson, T., et al. (2022). Treatment of coronary bifurcation lesions, part II: implanting two stents. The 16th expert consensus document of the European Bifurcation Club. EuroIntervention, 18(6), 457–470.