



Understanding Coronary Stent Thrombosis
Coronary stent thrombosis (ST) is one of the most serious complications following percutaneous coronary intervention (PCI). While modern drug-eluting stents (DES) have made the procedure incredibly safe, ST remains a high-stakes event, typically presenting as an acute myocardial infarction (STEMI) or sudden cardiac death.
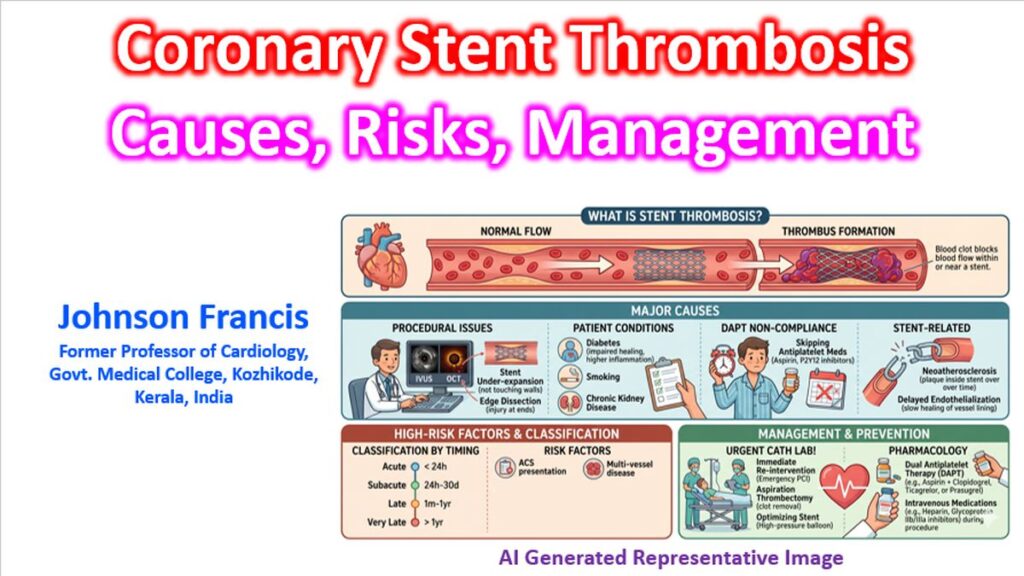
1. Classification by Timing
Stent thrombosis is categorized based on when it occurs after the initial procedure. This helps clinicians identify the most likely underlying cause.
| Category | Timing | Common Drivers |
| Acute | < 24 hours | Technical issues (dissection, under-expansion) |
| Subacute | 24 hours to 30 days | DAPT non-compliance, procedure-related issues |
| Late | 30 days to 1 year | Delayed endothelialization, hypersensitivity |
| Very Late | > 1 year | Neoatherosclerosis, stent fracture |
2. The Academic Definition (ARC Criteria)
To standardize research and clinical reporting, the Academic Research Consortium (ARC) defines ST by the level of certainty. The Academic Research Consortium is an informal collaboration between academic research organizations in the United States and Europe.
- Definite: Angiographic or pathologic confirmation of a thrombus.
- Probable: Any unexplained death within 30 days or acute MI in the territory of the stent without angiographic proof.
- Possible: Any unexplained death beyond 30 days.
3. Pathophysiology and Risk Factors
ST is rarely the result of a single factor; it usually involves a “perfect storm” of three categories:
Patient Factors
- Diabetes Mellitus: Increased platelet reactivity and impaired healing.
- Chronic Kidney Disease (CKD): Higher inflammatory state and calcified lesions.
- ACS Presentation: Patients stented during an acute coronary syndrome have a higher baseline risk than those with stable angina.
Procedural/Stent Factors
- Stent Under-expansion: The most common mechanical cause; it creates turbulent flow.
- Malapposition: The stent strut is not in contact with the vessel wall.
- Edge Dissection: Small tears at the ends of the stent that trigger the clotting cascade.
- Stent Length: Longer “full-metal jackets” increase the surface area for potential thrombosis.
Pharmacological Factors
- DAPT Non-compliance: Premature discontinuation of Dual Antiplatelet Therapy (Aspirin + a P2Y12 inhibitor) is the strongest predictor of early ST.
- Resistance: Genetic variations (e.g., CYP2C19 polymorphism) that make medications like Clopidogrel less effective.
4. Prevention and Management
Prevention
- Optimal Deployment: Using intravascular imaging (IVUS or OCT) to ensure the stent is fully expanded and apposed.
- DAPT Stewardship: Ensuring the patient understands the life-critical nature of their “blood thinners.”
- Potent P2Y12 Inhibitors: Using Ticagrelor or Prasugrel instead of Clopidogrel in high-risk ACS patients.
Management of Acute ST
If a patient presents with ST, it is a medical emergency requiring immediate return to the cath lab.
- Primary PCI: Emergent re-opening of the vessel.
- Thrombus Aspiration: Removing the clot manually if the burden is high.
- High-Pressure Ballooning: Correcting any underlying under-expansion.
- GP IIb/IIIa Inhibitors: Often used as “bailout” therapy to aggressively inhibit platelets during the procedure.
Clinical Note: While the incidence of ST has dropped significantly with second and third-generation DES (now roughly <1% at one year), the mortality rate of an ST event remains high, often cited between 10% and 25%.