



For most people, a patent foramen ovale (PFO) never needs to be closed. It is a common anatomical variant present in about 25% of the general population and is usually an incidental finding. However, over the last few years, some major clinical trials have shown that PFO closure is beneficial for a very specific subset of patients to prevent recurrent strokes.
Here is a breakdown of the current medical consensus on when PFO closure is needed and when it isn’t.
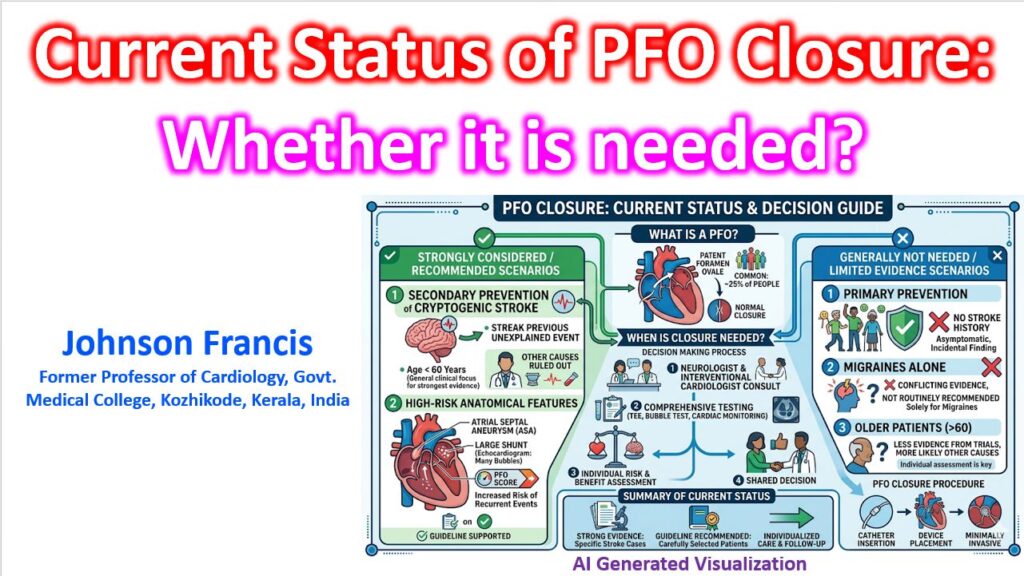
When PFO Closure is Strongly Indicated
The primary, evidence-based reason to close a PFO is for the secondary prevention of cryptogenic stroke (a stroke with no identifiable cause, also known as Embolic Stroke of Undetermined Source or ESUS).
Based on landmark trials like RESPECT, CLOSE, REDUCE, and DEFENSE-PFO, closure is generally recommended if the patient meets these criteria:
- Age: Typically under 60 years old.
- Event: Has suffered an ischemic stroke or transient ischemic attack (TIA) that is deemed cryptogenic after a thorough neurological and cardiac workup (e.g., ruling out carotid disease and atrial fibrillation).
- Anatomy: The PFO has “high-risk” anatomical features, such as a large right-to-left shunt or an associated Atrial Septal Aneurysm (ASA).
- RoPE Score: A high Risk of Paradoxical Embolism (RoPE) score (usually ≥7), which suggests the stroke was highly likely caused by a blood clot passing through the PFO rather than standard vascular disease. The RoPE score is a 10-point index designed to help distinguish whether a PFO in the setting of a cryptogenic stroke is pathogenic (the actual cause) or merely an incidental finding.
In these patients, combining a percutaneous device closure with antiplatelet therapy reduces the risk of recurrent stroke significantly more than medical therapy alone.
Rare but Acceptable Indications
Aside from stroke, there are a few specific scenarios where closure is considered:
- Platypnea-Orthodeoxia Syndrome: A rare condition where a patient experiences shortness of breath and a drop in blood oxygen levels when sitting or standing up, but not when lying down. PFO closure is often highly effective for this.
- Decompression Illness: Professional or frequent scuba divers who experience decompression sickness due to a PFO may undergo closure if they wish to continue deep diving without restrictions.
When PFO Closure is NOT Recommended
- Primary Prevention: Finding a PFO incidentally on an echocardiogram in someone who has never had a stroke or related symptoms does not warrant closure, regardless of the size of the PFO.
- Migraines: While observational data showed that some patients experienced relief from migraines with aura after a PFO closure, randomized controlled trials (like MIST, PRIMA, and PREMIUM) failed to prove that routine closure cures migraines. It is currently not recommended as a primary treatment for migraines.
- Older Patients (>60 years): Routine closure in older patients with a cryptogenic stroke is still debated. In this age group, occult atrial fibrillation is a much more likely cause of stroke than a PFO, so prolonged cardiac monitoring (like an implantable loop recorder) is usually required before a PFO is blamed.
Atrial Fibrillation – A Notable Risk!
PFO closure is generally a safe, minimally invasive transcatheter procedure (done through a vein in the groin) that takes less than an hour. Apart from the usual invasive procedure related risks, the most notable risk associated with the procedure is a higher incidence of new-onset Atrial Fibrillation (AFib) following the device implantation seen in some studies. Trials showed an AFib rate of roughly 4% to 6% post-procedure, which is why careful patient selection and post-procedure rhythm monitoring are crucial.