


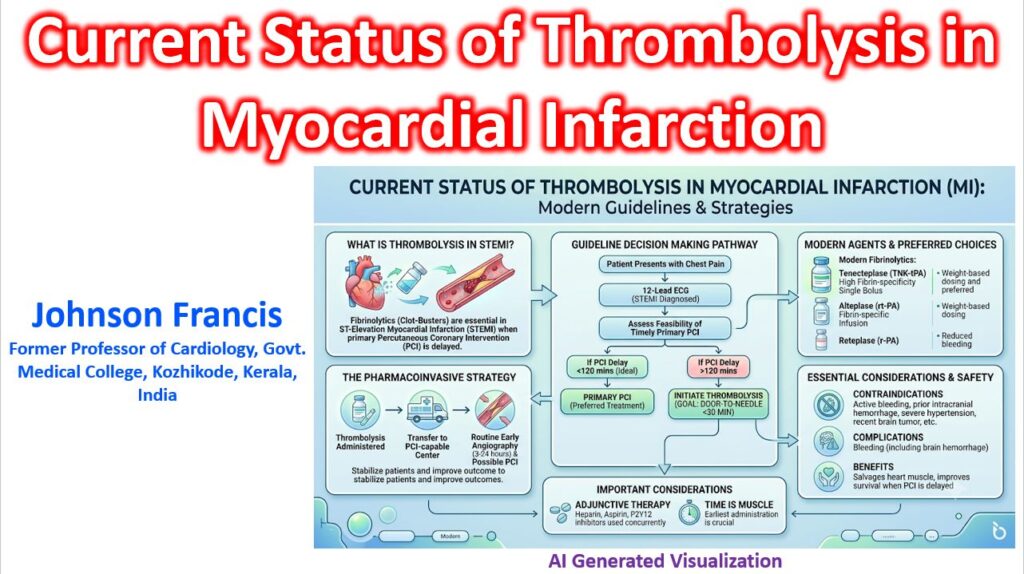
In contemporary clinical cardiology, systemic thrombolysis (fibrinolysis) has shifted from being treated as a standalone reperfusion endpoint into the Pharmacoinvasive Strategy. While Primary Percutaneous Coronary Intervention (pPCI) remains the definitive Class I reperfusion standard for ST-Segment Elevation Myocardial Infarction (STEMI), fibrinolysis remains the essential first-line reperfusion vector whenever timely mechanical reperfusion is unfeasible—particularly in geographically dispersed regions, and non-pPCI capable facilities.
Guideline Decision Matrix & Timelines
Current European Society of Cardiology (ESC) and American College of Cardiology/American Heart Association (ACC/AHA) guidelines enforce strict temporal metrics to minimize total ischemic time:
- The 120-Minute Gate: When a patient presents to a non-pPCI capable facility or emergency medical services (EMS), the clinical team must calculate anticipated delay. If time from First Medical Contact (FMC) to cath lab wire crossing is anticipated to exceed 120 minutes, fibrinolytic therapy must be initiated immediately.
- Door-to-Needle Benchmark: When indicated, lytic administration should occur within 30 minutes of hospital arrival, or ideally in the field via prehospital EMS protocols.
- The Transfer Mandate: Standalone thrombolysis without subsequent institutional transfer is obsolete. Every lysed patient must be systematically transferred to a PCI-capable hub as early as feasible.
The Pharmacoinvasive Mandate
Once fibrinolysis is administered, post-lytic clinical triage dictates the catheterization laboratory schedule:
- Rescue PCI (Immediate): Mandated if fibrinolysis fails. Failure is defined clinically by less than 50% ST-segment resolution at 60 to 90 minutes post-bolus, persistent hemodynamic instability, cardiogenic shock, or ongoing ischemic chest pain.
- Routine Early Angiography (3 to 24 Hours): Mandated for all patients with clinically successful reperfusion.
Critical Window Nuance: Performing routine angiography under 2 to 3 hours post-successful lysis significantly elevates access-site and systemic bleeding risks without improving infarct-related artery (IRA) patency. Conversely, delaying beyond 24 hours forfeits the opportunity to secure the residual unstable plaque before reocclusion occurs.
Pharmacological Evolution: Tenecteplase
Third-generation Tenecteplase (TNK-tPA) has firmly supplanted second-generation alteplase and first-generation streptokinase as the global standard of care. Engineered via three specific amino acid substitutions on the human tissue plasminogen activator backbone, TNK offers distinct pharmacokinetic advantages:
| Clinical Attribute | Tenecteplase (TNK-tPA) | Alteplase (rt-PA) |
| Administration | Single weight-adjusted IV bolus (5–10 sec) | Front-loaded bolus + 90-minute infusion |
| Fibrin Specificity | High (14-fold greater than native tPA) | Moderate |
| Plasma Half-Life | 20 to 24 minutes | 4 to 5 minutes |
| PAI-1 Resistance | High (80-fold greater resistance) | Highly susceptible to rapid inhibition |
| TIMI 3 Patency Rate | 60% to 65% at 90 minutes | 50% to 60% at 90 minutes |
The single-bolus dynamic of TNK is transformative for prehospital care, allowing solo paramedics or rural physicians to execute rapid reperfusion without managing complex, fragile weight-based IV infusion pumps during transport.
Contemporary Adjunctive Pharmacotherapy
Fibrinolysis exposes highly thrombogenic plaque core surfaces and triggers paradoxical thrombin activation. Achieving lasting vessel patency requires aggressive adjunctive antithrombotic coverage:
- Dual Antiplatelet Therapy (DAPT): Aspirin combined with Clopidogrel. Important: Newer potent P2Y12 inhibitors (Prasugrel and Ticagrelor) are contraindicated at the exact time of fibrinolysis due to unacceptable intracranial hemorrhage (ICH) risk, though downstream switching post-angiography is common.
- Anticoagulation: Intravenous Enoxaparin is superior to unfractionated heparin (UFH) for preventing IRA reocclusion. Dosing must be strictly adjusted for patients over 75 years old and severe renal impairment.
Emerging Frontiers
- Intracoronary Lysis During pPCI: In cases of massive thrombotic burden during mechanical intervention, low-dose intracoronary tenecteplase or alteplase is gaining clinical traction as an adjunctive bailout to dissolve microvascular emboli and resolve slow-flow or no-reflow phenomena.
- AI-Triaged Prehospital Networks: The expansion of cloud-connected 12-lead ECG transmission analyzed instantly by remote AI algorithms is compressing diagnostic delays, shifting the therapeutic goalpost from “door-to-needle” to “first contact-to-needle” directly at the patient’s bedside.