Detection of myocardial infarction in paced rhythm
Detection of myocardial infarction in paced rhythm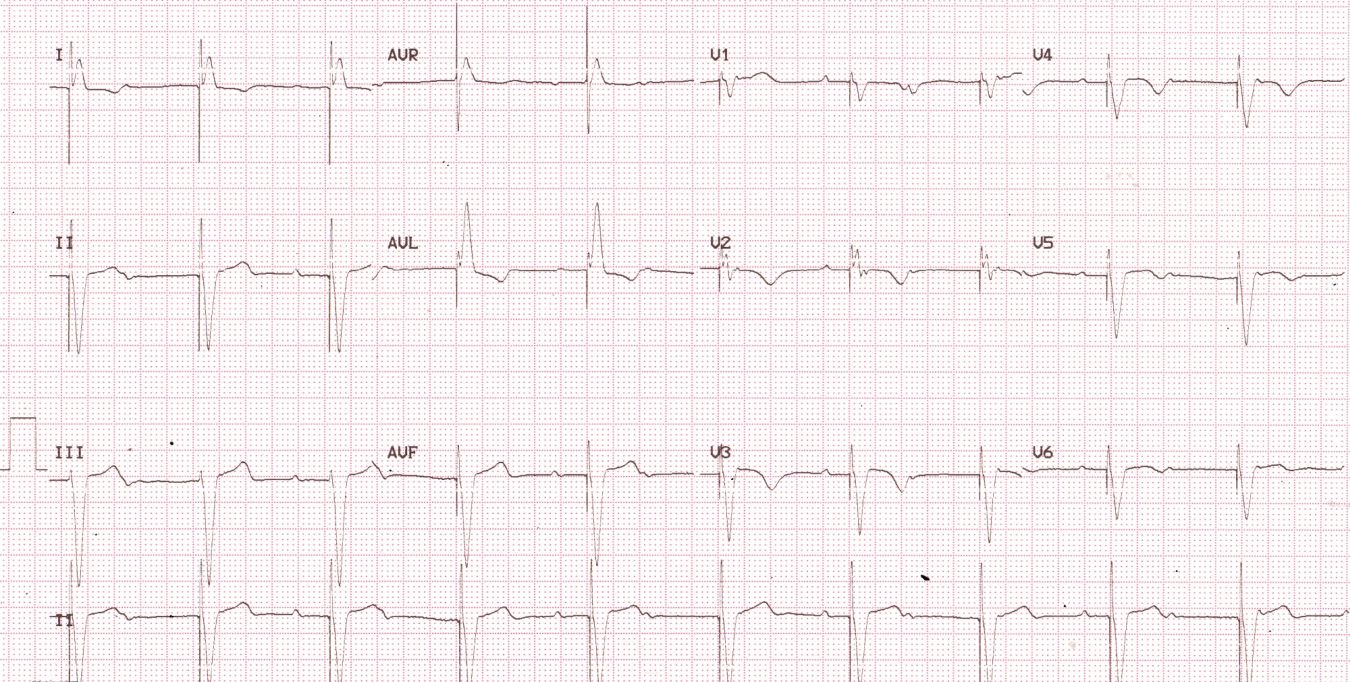
Detection of myocardial infarction in paced rhythm is often difficult due to the baseline abnormality in depolarization and secondary abnormality in repolarization. But if an ECG prior to myocardial infarction is available, careful lead by lead comparison will make detection of a fresh myocardial infarction rather easy. This should of course be complemented by clinical evaluation and estimation of biomarkers of myocardial necrosis. Large amplitude pacing spikes are seen before each QRS complex indicating unipolar ventricular pacing. Bipolar ventricular pacing will show small pacing spikes as the circuit is completed locally near the site of pacing while in unipolar pacing the metallic can of the pacemaker acts as the positive electrode. Hence the pacing circuit is large from the tip of the pacing electrode which is cathode to the metallic can of the pacemaker housing, through the body. Lead I and aVL shows left bundle branch block pattern and inferior leads show negative QRS complexes. Together these patterns suggest pacing from the right ventricular apex. Dissociated P waves suggest complete heart block as the reason for pacemaker implantation. T waves are inverted in leads V2-V6, in the presence of negative QRS complexes (concordant T waves). This would suggest a primary T wave abnormality.
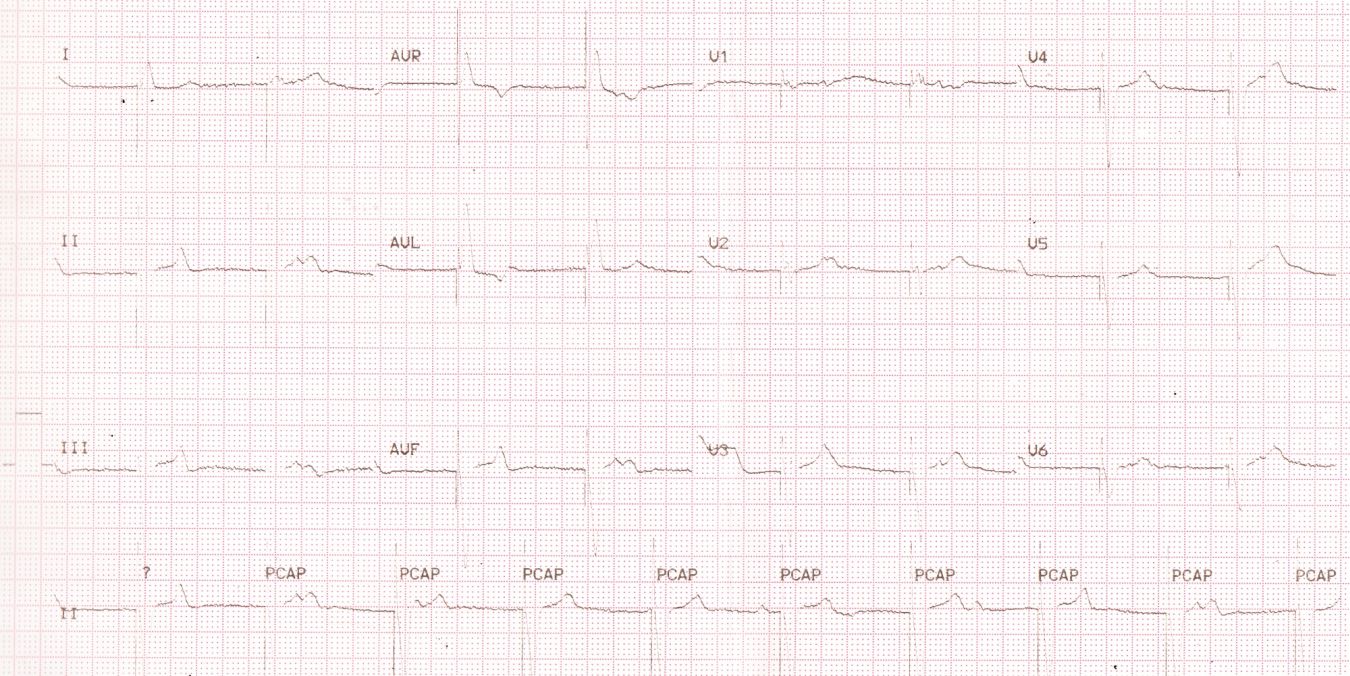
Review of previous ECG, though partially faded, showed upright T waves in anterior leads. This in addition to the clinical history of anginal pain, wall motion abnormality on echo and elevated troponins confirmed the possibility of an anterior myocardial infarction.
Kozlowski FH and colleagues have suggested that any difference from the anticipated ST-T pattern in the paced rhythm can be considered for the diagnosis of myocardial infarction in the appropriate clinical setting even if the previous ECG is not available for comparison [1].
Another interesting report was on ST elevation myocardial infraction in the presence of biventricular paced rhythm [2]. In that case, ECG had evidence of biventricular paced rhythm with superimposed ST segment elevations in anterolateral leads indicative of myocardial injury. Patient had a total occlusion of proximal left anterior descending coronary artery for which angioplasty and stenting was done.
Sgarbossa EB et al had found 17 cases with right ventricular paced rhythm suitable for analysis among 41,021 patients with enzymatically confirmed myocardial infarction in the GUSTO trial [3]. They found that discordant ST elevation of 5 mm or more, concordant ST elevation of 1 mm or more and ST depression of 1 mm or more in leads V1, V2, V3 were the most useful in early diagnosis of myocardial infarction in the presence of right ventricular paced rhythm.
Abraham AS et found the Sgarbossa criteria useful in their patient with re-infarction due to stent thrombosis [4]. Their patient had discordant ST segment elevation greater than 5 mm in leads V3, V4 and concordant ST segment elevation greater than 1 mm in lead V6.
References
- Kozlowski FH, Brady WJ, Aufderheide TP, Buckley RS. The electrocardiographic diagnosis of acute myocardial infarction in patients with ventricular paced rhythms. Acad Emerg Med. 1998 Jan;5(1):52-7.
-
Karumbaiah K, Omar B. ST-elevation myocardial infarction in the presence of biventricular paced rhythm. J Emerg Med. 2013 Aug;45(2):e35-40. doi: 10.1016/j.jemermed.2013.03.034. Epub 2013 Jun 12. PMID: 23769390.
- Sgarbossa EB, Pinski SL, Gates KB, Wagner GS. Early electrocardiographic diagnosis of acute myocardial infarction in the presence of ventricular paced rhythm. GUSTO-I investigators. Am J Cardiol. 1996 Feb 15;77(5):423-4. doi: 10.1016/s0002-9149(97)89377-0. PMID: 8602576.
- Abraham AS, Vinson DR, Levis JT. ECG Diagnosis: Acute Myocardial Infarction in a Ventricular-Paced Rhythm. Perm J. 2019;23:19-001. doi: 10.7812/TPP/19-001. Epub 2019 Jun 27. PMID: 31314731; PMCID: PMC6636527.
Related Posts


About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal