Dextrocardia and dextroposition
Dextrocardia and dextroposition
Here we have two X-rays illustrating dextrocardia and dextroposition. First one is true dextrocardia with situs inversus while the second is dextroposition in left sided pleural effusion.
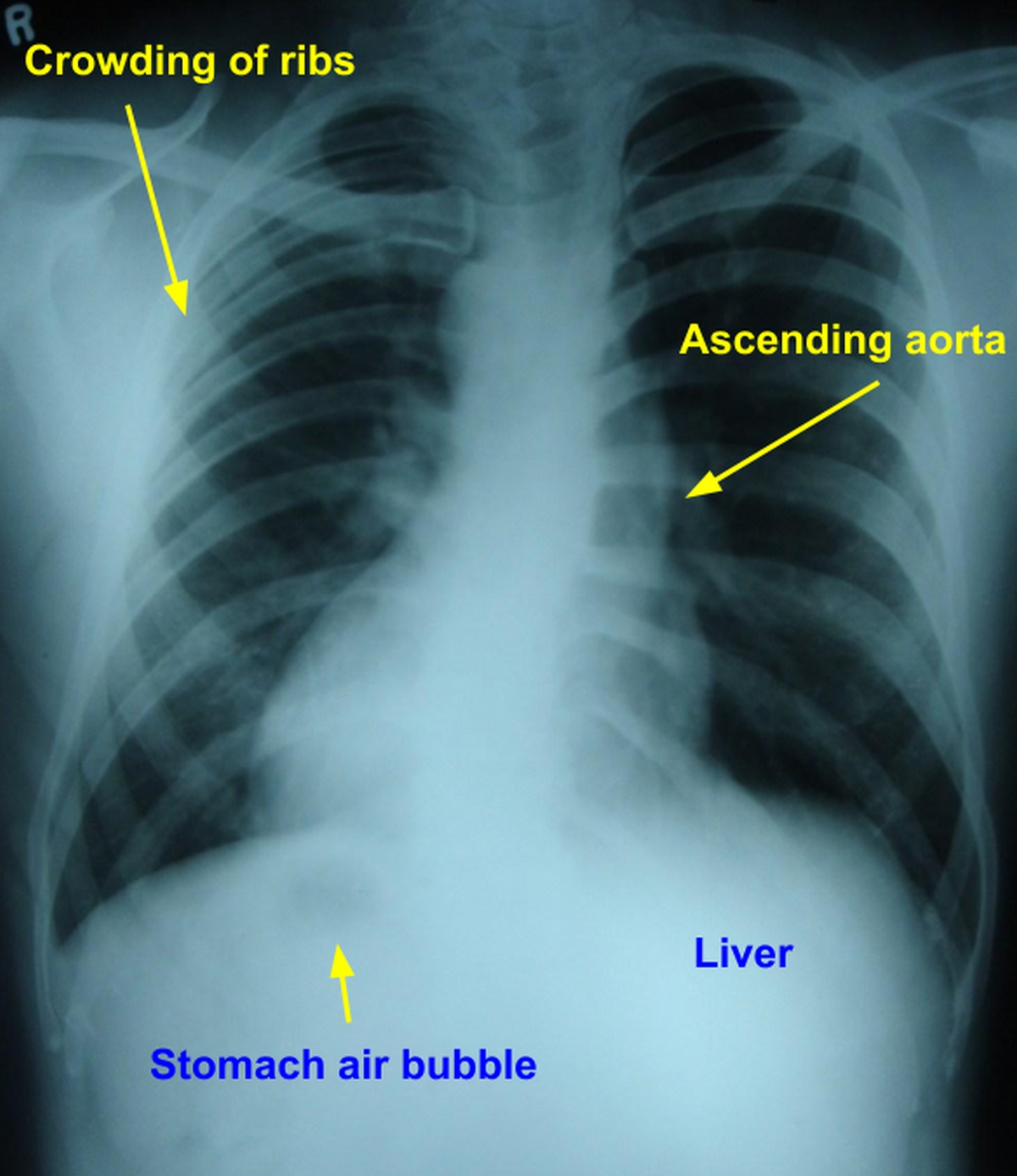
Dextrocardia with situs inversus
Dextrocardia is evident as the apex is pointing to the right and the right atrial contour is on the left. The gastric air bubble is on the right (below the diaphragm) and liver shadow on the left, indicating situs inversus. The ascending aortic shadow on the left is a little prominent. There is mild scoliosis with convexity to the left which could be partly positional. Crowding of upper ribs on the right side could be due to the scoliosis.
Adolescent idiopathic scoliosis affects 2 to 3% of general population. 80 – 99% show right thoracic curve convexity [1]. Compton J et al noted 19 patients with adolescent idiopathic scoliosis with Cobb angle > 10° among 110 patients with dextrocardia. 15 of them had left sided thoracic curvature, which is similar to that seen in the chest X-ray shown above. Of the 6 patients with normal abdominal organ orientation, 5 had left sided thoracic curvature. Authors concluded that thoracic organ orientation affects the direction of convexity of scoliosis. Left sided thoracic curvature with dextrocardia may not be associated with intra spinal pathology [1].
Kartagener’s syndrome with situs inversus, sinusitis and bronchiectasis is an important association of dextrocardia [2]. In males it is associated with infertility because spermatozoa are immotile due to primary ciliary dyskinesia. Primary ciliary dyskinesia is transmitted in a recessive pattern and 50% have situs inversus totalis and Kartagener’s syndrome [3].
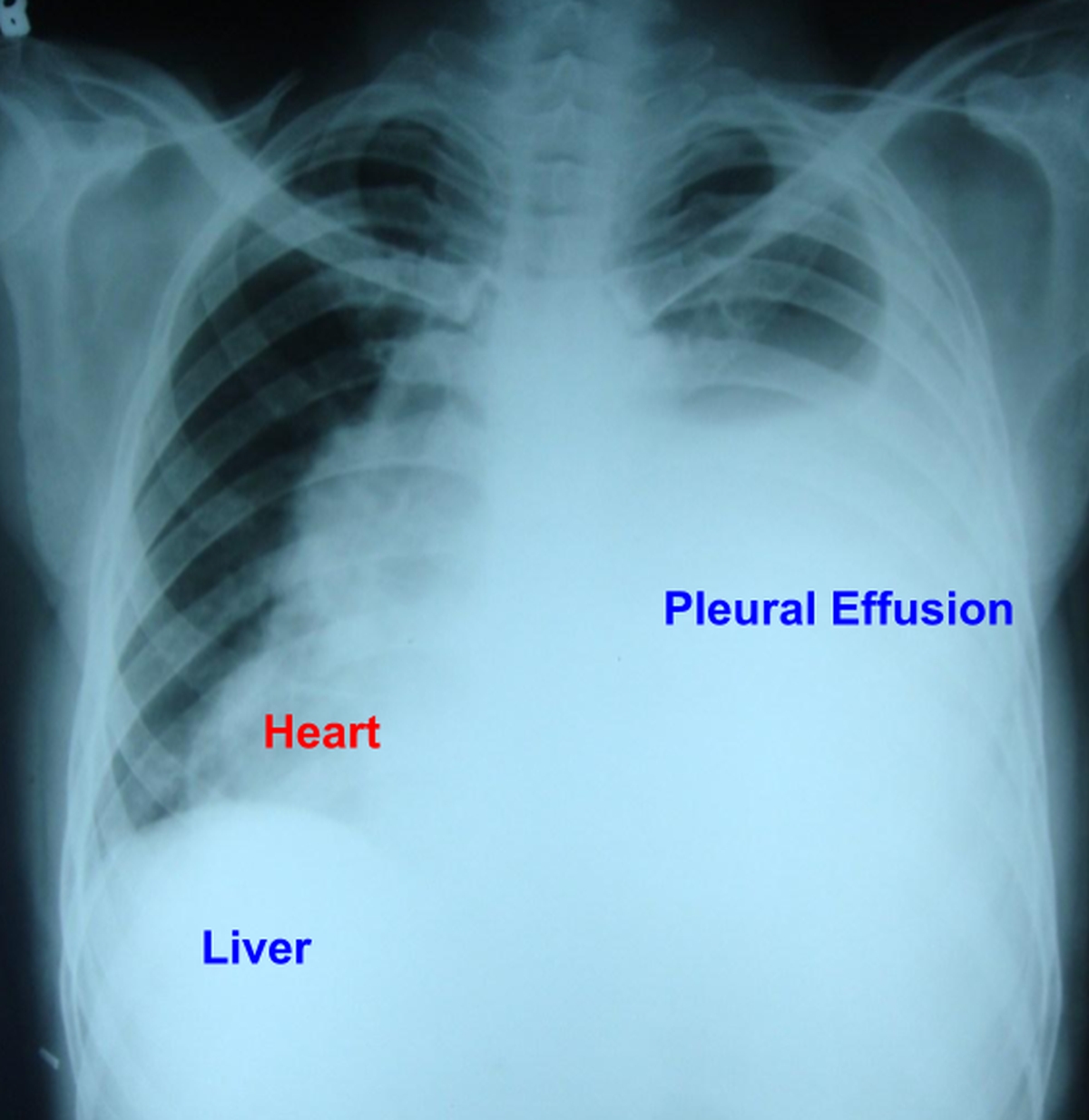
Left sided pleural effusion with dextroposition
There is massive pleural effusion on the left side pushing the heart along with the mediastinum to the right side producing a dextroposition. The higher level of the effusion in the axilla is evident. The liver shadow is on the right side indicating situs solitus. Stomach air bubble is not visible well.
Dextroposition of the heart can also be due to congenital hypoplasia of right lung [4,5].
References
- Compton J, Voort WV, Weinstein S. Scoliosis Curvature Follows Thoracic Organ Orientation. Spine (Phila Pa 1976). 2020 Mar 15;45(6):378-380.
- Gupta S, Handa KK, Kasliwal RR, Bajpai P. A case of Kartagener’s syndrome: Importance of early diagnosis and treatment. Indian J Hum Genet. 2012 May;18(2):263-7.
- Kennedy MP, Omran H, Leigh MW, Dell S, Morgan L, Molina PL, Robinson BV, Minnix SL, Olbrich H, Severin T, Ahrens P, Lange L, Morillas HN, Noone PG, Zariwala MA, Knowles MR. Congenital heart disease and other heterotaxic defects in a large cohort of patients with primary ciliary dyskinesia. Circulation. 2007 Jun 5;115(22):2814-21.
- Wang Y, Yang X, Dong L, Shu X. A curious case of cardiac dextroposition. Eur Heart J. 2014 May;35(18):1185.
- Baranchuk A, Somani R, Simpson CS, Michael KA, Redfearn DP. Ablation of a left lateral accessory pathway in a patient with dextroposition of the heart. Cardiol J. 2012;19(4):439-40.
Related Posts


About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal