



The diagnosis and management of Athlete’s Heart hinges on distinguishing benign, exercise-induced cardiac remodeling from structural cardiomyopathies that predispose patients to sudden cardiac death (SCD). The physiological adaptations can overlap significantly with conditions like hypertrophic cardiomyopathy (HCM), dilated cardiomyopathy (DCM), and arrhythmogenic right ventricular cardiomyopathy (ARVC) in the clinical “grey zones.”
Pathophysiology of Remodeling
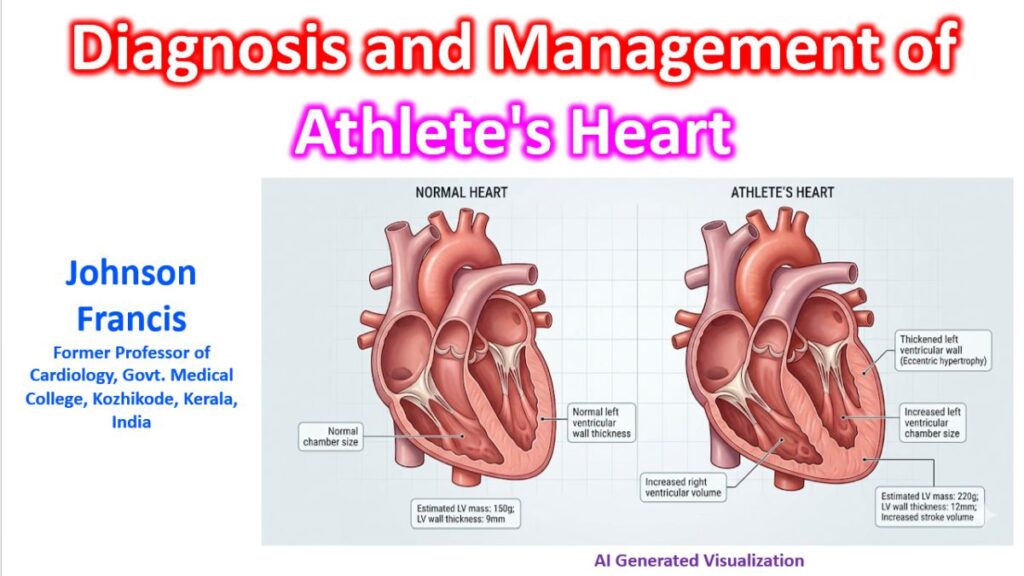
Exercise type drives the morphological changes in the myocardium:
- Endurance sports (Dynamic load): Induce eccentric hypertrophy characterized by biventricular dilation, increased stroke volume, and proportional increases in wall thickness.
- Strength sports (Static load): Induce concentric hypertrophy with increased wall thickness but mild or absent ventricular dilation.
Diagnostic Evaluation
When evaluating an athlete, a comprehensive multimodal approach is standard to avoid misdiagnosis, which can lead to false reassurance or unnecessary exclusion from sports.
1. 12-Lead ECG
The 12-lead ECG is highly sensitive (over 95%) for identifying pathological conditions like HCM. The core challenge is differentiating training-related adaptations (e.g., sinus bradycardia, high voltage QRS without unusual features, first-degree AV block) from borderline or outright abnormal findings (e.g., deep T-wave inversions, ST-segment depression, pathologic Q waves).
Key insight: Finding borderline or abnormal ECG changes should trigger immediate secondary evaluation, usually beginning with echocardiography.
2. Echocardiography and CMR
Conventional echocardiography is the first-line imaging modality to assess wall thickness, cavity dimensions, and diastolic function. If findings remain equivocal, Cardiovascular Magnetic Resonance (CMR) is crucial. CMR provides precise tissue characterization to identify late gadolinium enhancement (LGE) — a hallmark of fibrosis seen in cardiomyopathy but absent in pure physiologic adaptation.
Differentiating Pathological Mimics
The overlapping phenotypes create diagnostic grey zones. The table below outlines parameters used to distinguish physiologic remodeling from the most common structural mimics.
| Parameter | Athlete’s Heart | Hypertrophic Cardiomyopathy | Dilated Cardiomyopathy |
| LV Wall Thickness | Symmetrical, homogenous (<15 mm) | Asymmetrical, heterogenous (>15 mm) | Normal or thinned |
| LV Cavity Size | Enlarged (>55 mm) | Small or normal (<45 mm) | Enlarged (>55 mm) |
| Diastolic Function | Normal to supranormal | Impaired relaxation | Variable |
| Exercise Response | Excellent reserve (LVEF increases >10%) | Dynamic LV outflow tract obstruction | Blunted stroke volume increase |
| CMR Findings | No fibrosis / no LGE | LGE often present | LGE often present |
| Deconditioning | LVH regresses after 1-3 months | No structural regression | No structural regression |
Management and Return-to-Play
If the diagnosis firmly points to physiologic Athlete’s Heart, no specific treatment is required, and the athlete is cleared for full participation.
For cases remaining in the grey zone despite advanced imaging, a brief period of detraining (deconditioning) for 1 to 3 months can serve as a diagnostic tool. In true Athlete’s Heart, left ventricular hypertrophy and cavity dilation will regress; pathological remodeling will persist.