



Temporary cardiac pacing is a critical intervention for hemodynamically unstable bradyarrhythmias, typically serving as a rapid bridge to permanent pacemaker implantation or the resolution of a transient conduction block (e.g., drug toxicity, inferior STEMI).
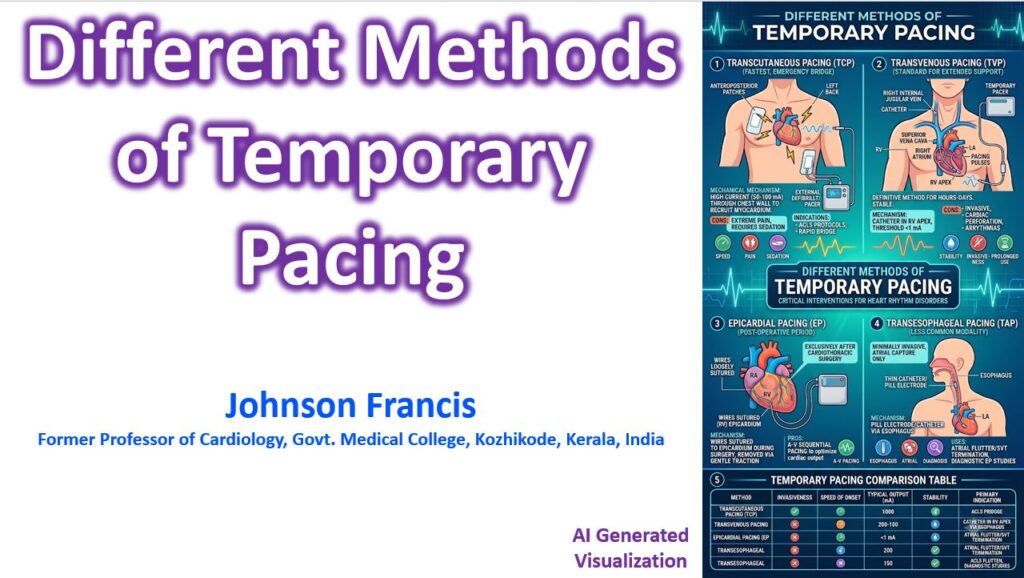
1. Transcutaneous Pacing (TCP)
The fastest, least invasive method, utilized in emergency settings (ACLS protocol) as a first-line bridge.
- Mechanism: Large adhesive electrodes are placed on the chest wall. Anteroposterior placement is ideal to minimize transthoracic impedance and recruit the maximum amount of myocardium.
- Settings: Requires high current outputs (often 50–100 mA) to achieve ventricular capture through the chest wall and skeletal muscle.
- Clinical Caveats: It causes severe skeletal muscle contraction and is highly painful. Conscious patients require aggressive sedation and analgesia. Mechanical capture must be verified by assessing central pulses (like the femoral), as the electrical artifact can mimic capture on the monitor, and peripheral pulses may simply reflect skeletal muscle twitching.
2. Transvenous Pacing (TVP)
The definitive standard for temporary pacing when prolonged support (hours to days) is required.
- Mechanism: A pacing catheter is advanced via central venous access and lodged in the right ventricular apex. The right internal jugular is often preferred due to a straight anatomical path to the RV, followed by the left subclavian or femoral veins.
- Settings: Once positioned under fluoroscopy or ECG guidance, the pacing threshold is identified (usually <1.0 mA). The output is typically set at 2–3 times the threshold to ensure an adequate safety margin.
- Clinical Caveats: TVP offers stable, reliable pacing with minimal patient discomfort once placed. However, it carries risks associated with central line placement, cardiac perforation (especially in a recently infarcted RV), and catheter-induced ventricular arrhythmias during insertion.
3. Epicardial Pacing
Used almost exclusively in the immediate post-operative period following cardiothoracic surgery.
- Mechanism: During open-heart surgery, bipolar or unipolar wires are loosely sutured directly to the epicardium of the right atrium, right ventricle, or both. The wires are exteriorized through the chest wall and connected to an external generator.
- Clinical Caveats: This method allows for A-V sequential pacing to optimize cardiac output in the vulnerable post-bypass period. When no longer needed, the wires are simply removed via gentle transcutaneous traction.
4. Transesophageal Pacing (TAP)
A less common, non-invasive method utilizing the anatomical proximity of esophagus to the left atrium.
- Mechanism: A pill-electrode is swallowed or placed via a nasogastric tube until it sits directly posterior to the left atrium.
- Clinical Caveats: Due to the physical distance to the ventricles, it can reliably capture only the atria. It is primarily used for overdrive pacing to terminate atrial flutter or SVT, or for diagnostic electrophysiology studies in pediatric population.