



When a patient presents with a regular or irregular tachycardia and a narrow QRS complex (less than 120 milliseconds), it tells us that ventricular depolarization is occurring via the normal, rapid His-Purkinje system. This almost always points to an origin above or within the Bundle of His—collectively categorized as Supraventricular Tachycardias (SVT).
The most practical clinical approach to narrowing down the differential diagnosis is to first assess regularity, and then evaluate the relationship between the P waves and QRS complexes.
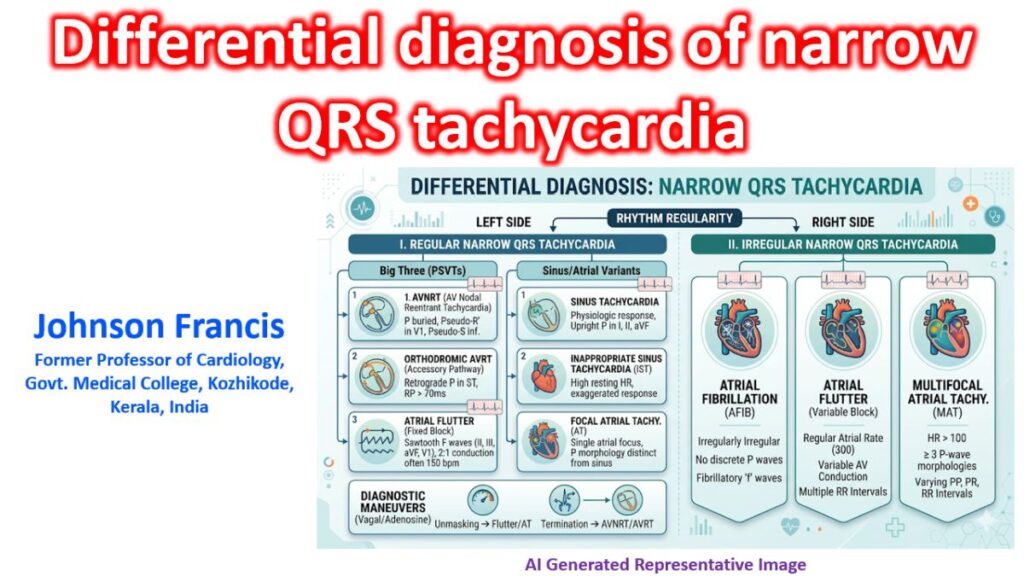
1. Regular Narrow QRS Tachycardia
If the R-R intervals are perfectly regular, the differential largely narrows down to three primary culprits, alongside a few distinct sinus variants.
The Big Three (Paroxysmal SVTs)
- AV Nodal Reentrant Tachycardia (AVNRT): The most common regular SVT. It utilizes a dual-pathway system within the AV node (slow and fast pathways). Because ventricles and atria are activated nearly simultaneously, P waves are typically buried inside the QRS complex or appear as a “pseudo-R'” in lead V1 or a “pseudo-S” in the inferior leads.
- AV Reentrant Tachycardia (AVRT): This relies on an anatomically distinct accessory pathway (like in Wolff-Parkinson-White syndrome) creating a macro-reentrant circuit.
- Orthodromic AVRT: Conduction goes down the AV node (keeping the QRS narrow) and back up the accessory pathway. P waves are usually clearly visible in the ST segment, retrogradely inverted in inferior leads, with an RP interval greater than 70 ms.
- Atrial Flutter (with fixed block): Typically presents with a classic ventricular rate of 150 bpm (2:1 conduction of a ~300 bpm atrial rate). Look closely at leads II, III, aVF, and V1 for the characteristic sawtooth “F” waves, especially if the rate refuses to budge.
Sinus and Atrial Variants
- Sinus Tachycardia: A normal physiologic response to stress, pain, hypovolemia, or fever. It features a normal, upright P-wave morphology in leads I, II, and aVF preceding every QRS.
- Inappropriate Sinus Tachycardia (IST): An elevated resting heart rate greater than 100 bpm or exaggerated response to minimal exertion without an identifiable physiological trigger, keeping identical normal sinus P-wave morphology.
- Sinoatrial Nodal Reentrant Tachycardia (SANRT): A paroxysmal micro-reentrant tachycardia arising near the sinus node. It mimics sinus tachycardia perfectly on the ECG but starts and stops abruptly.
- Focal Atrial Tachycardia (AT) with fixed block: Arises from a distinct atrial focus outside the SA node. The P wave morphology will differ from normal sinus rhythm (e.g., inverted in lead I or aVL if originating from the left atrium).
2. Irregular Narrow QRS Tachycardia
When the R-R intervals are variable, the differential shifts completely toward atrial arrhythmias with variable conduction through the AV node.
- Atrial Fibrillation (AFib): The quintessential “irregularly irregular” rhythm. There are no discernible, organized P waves; instead, the baseline shows chaotic fibrillatory (“f”) waves.
- Atrial Flutter with Variable Conduction: The macro-reentrant atrial circuit remains completely regular (~300 bpm), but the AV node blocks the impulses unpredictably (e.g., alternating between 2:1, 3:1, and 4:1 conduction), creating an irregular ventricular response.
- Multifocal Atrial Tachycardia (MAT): Defined by a heart rate greater than 100 bpm with three or more distinct P-wave morphologies within a single lead, and varying PP, PR, and RR intervals. This is highly associated with severe underlying pulmonary disease (like severe COPD exacerbations).
The Electrocardiographic Roadmap (Regular R-R)
To quickly differentiate the regular narrow QRS tachycardias on an ECG, we look at the location of the retrograde P wave relative to the QRS complexes:
| RP Classification | Timing | Primary Differentials | Key ECG Clue |
| P buried / Pseudo-R’ | RP < 70 ms | Typical AVNRT | Pseudo-R’ in V1 or pseudo-S in inferior leads that disappears in sinus rhythm. |
| Short RP | 70 ms < RP < PR | Orthodromic AVRT, Atrial Tachycardia | Retrograde P wave visible in the ST segment, well after the QRS ends. |
| Long RP | RP > PR | Atypical AVNRT, Atrial Tachycardia, Permanent Junctional Reciprocating Tachycardia (PJRT) | P wave falls before the next QRS, often masquerading as a prolonged sinus PR interval. |
Diagnostic Bedside Maneuvers
When the baseline ECG doesn’t provide an absolute answer because the rate is too fast to clearly map the P waves, two main interventions can unmask the underlying rhythm:
- Vagal Maneuvers: Valsalva or carotid sinus massage increases vagal tone to transiently slow AV nodal conduction.
- Adenosine: A rapid intravenous bolus blocks conduction through the AV node for a few seconds.
The Diagnostic Response:
- If the rhythm abruptly terminates back to sinus rhythm, the AV node is an essential limb of the reentrant circuit (highly suggestive of AVNRT or AVRT).
- If the rhythm transiently slows down, unmasking underlying rapid atrial activity (sawtooth waves or flutter waves) without stopping the atrial arrhythmia itself, the mechanism is Atrial Flutter or Atrial Tachycardia.