


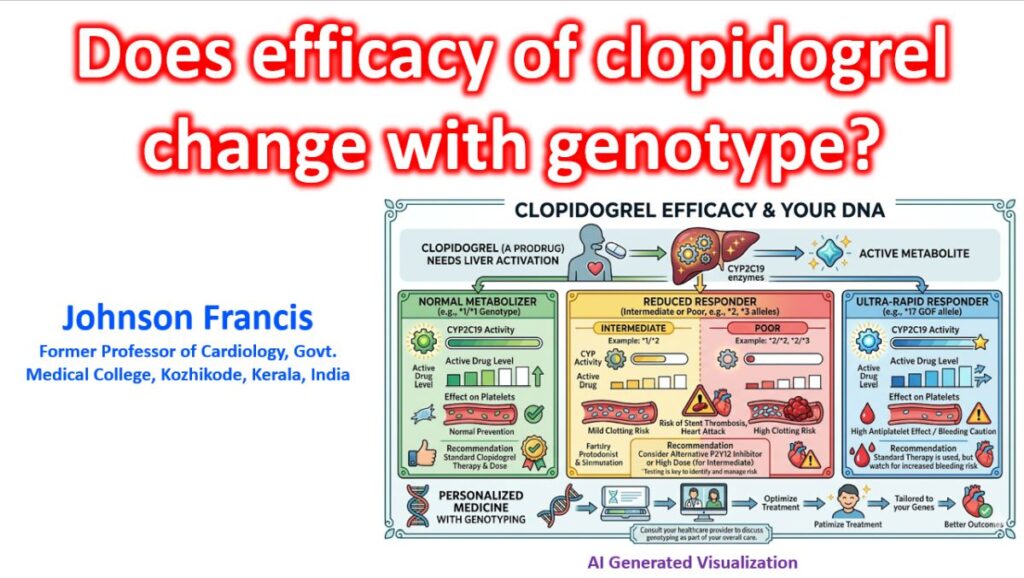

Yes, the efficacy of clopidogrel is highly dependent on genotype, specifically regarding the CYP2C19 gene. Because clopidogrel is a thienopyridine prodrug, it requires a two-step hepatic biotransformation to become its active thiol metabolite, which then irreversibly binds to the platelet P2Y12 receptor. The CYP2C19 enzyme is the primary catalyst for both of these critical metabolic steps.
The CYP2C19 Alleles and Phenotypes
Genetic polymorphisms in the CYP2C19 gene dictate the liver’s ability to generate the active metabolite. The alleles are generally categorized into wild-type (normal), loss-of-function (LOF), and gain-of-function (GOF).
- CYP2C19*1: The wild-type allele (normal enzymatic function).
- CYP2C19*2 and *3: The most common loss-of-function (LOF) alleles. The *2 allele is common across most populations, while *3 is seen frequently in Asian demographics.
- CYP2C19*17: A gain-of-function (GOF) allele that leads to increased transcription and ultra-rapid metabolism.
Key insight: Carriers of LOF alleles (Intermediate and Poor Metabolizers) experience high on-treatment platelet reactivity (HPR) when given standard doses of clopidogrel, making them clinically resistant to the drug.
Clinical Implications in Cardiology
The impact of genotype is most pronounced in high-risk scenarios, particularly for patients undergoing percutaneous coronary intervention (PCI) for acute coronary syndromes (ACS).
The Risk of Adverse Events
Patients with one or two LOF alleles who are treated with clopidogrel post-PCI have a significantly increased risk of major adverse cardiovascular events (MACE). Most critically, they have a demonstrably higher rate of stent thrombosis compared to normal metabolizers.
Management Guidelines
The Clinical Pharmacogenetics Implementation Consortium (CPIC) provides explicit guidance regarding clopidogrel use based on CYP2C19 genotype:
- Poor and Intermediate Metabolizers (LOF carriers): Guidelines strongly recommend utilizing an alternative P2Y12 inhibitor—specifically prasugrel or ticagrelor. These agents are either less dependent (prasugrel) or entirely independent (ticagrelor, which is active as administered) of CYP2C19 metabolism.
- Ultra-Rapid Metabolizers (GOF carriers): These patients form abundant active metabolite. While they receive excellent ischemic protection, they may face an increased risk of bleeding. Standard dosing is generally maintained, but bleeding risk must be monitored.
While routine, universal CYP2C19 genotyping is not standard across all practices, genotype-guided P2Y12 de-escalation strategies (as explored in trials like TAILOR-PCI and POPULAR GENETICS) are increasingly utilized to optimize the balance between ischemic and bleeding risks after PCI.
Review of Two Landmark Clinical Trials
TAILOR-PCI and POPULAR GENETICS are the two landmark trials which serve as the foundational pillars for genotype-guided antiplatelet therapy in modern cardiology. They elegantly represent two sides of the same precision-medicine coin: TAILOR-PCI explored an escalation strategy relative to a clopidogrel standard, while POPULAR GENETICS explored a de-escalation strategy relative to a potent P2Y12 standard.
1. TAILOR-PCI (The “Escalation” Strategy)
This trial investigated whether identifying CYP2C19 loss-of-function (LOF) carriers and escalating them to ticagrelor would improve outcomes compared to standard, universal clopidogrel therapy.
- Population: Over 5,000 patients with ACS or stable CAD undergoing PCI.
- Design:
- Genotype-Guided Arm: Point-of-care testing was performed. Patients with CYP2C19 LOF alleles (*2 or *3) received ticagrelor. Wild-type patients received clopidogrel.
- Control Arm: Standard care with universal clopidogrel for all patients (genotype blinded for 1 year).
- Primary Endpoint: 1-year MACE (cardiovascular death, myocardial infarction, stroke, stent thrombosis, or severe recurrent ischemia).
- The Results & Nuance:
- The trial technically missed its primary endpoint for statistical significance at 1 year. The genotype-guided strategy showed a 34% reduction in MACE among LOF carriers, but the p-value was borderline (Hazard Ratio 0.66; 95% CI, 0.43-1.02; p=0.06).
- The Clinical Catch: A prespecified analysis looking at the first 3 months post-PCI—the period of highest thrombotic risk—showed a highly significant 79% reduction in adverse events for the genotype-guided group. While strictly a negative trial at 1 year, the strong trend and early benefit heavily support the biological premise of genotyping.
2. POPULAR GENETICS (The “De-escalation” Strategy)
Because potent P2Y12 inhibitors (ticagrelor and prasugrel) reduce ischemic events but significantly increase bleeding risk, this trial sought to safely step down therapy for patients without LOF alleles.
- Population: Almost 2,500 patients with STEMI undergoing primary PCI.
- Design:
- Genotype-Guided Arm: Patients underwent testing. If they carried a LOF allele, they received standard potent agents (ticagrelor/prasugrel). If they were wild-type (normal metabolizers), therapy was de-escalated to clopidogrel.
- Control Arm: Universal treatment with a potent P2Y12 inhibitor (ticagrelor or prasugrel) for all patients.
- Primary Endpoints: A non-inferiority design for net adverse clinical events (NACE: death, MI, definite stent thrombosis, stroke, or PLATO major bleeding) and a superiority design for bleeding (PLATO major and minor).
- The Results & Nuance:
- Ischemia: The genotype-guided de-escalation strategy was non-inferior to standard potent therapy for ischemic events (NACE occurred in 5.1% of the guided group vs. 5.9% of the standard group).
- Bleeding: The guided strategy was superior for safety, significantly reducing PLATO major and minor bleeding (9.8% vs. 12.5%).
- The Clinical Catch: This trial solidified the concept that standardizing potent agents for everyone exposes wild-type patients to unnecessary bleeding risks without added ischemic benefit.
The Clinical Bottom Line
When presented together, these trials build a compelling narrative for personalized medicine in the cath lab:
- If the baseline is Clopidogrel: Genotyping identifies the ~30% of patients who desperately need escalation to avoid stent thrombosis (TAILOR-PCI).
- If the baseline is Ticagrelor/Prasugrel: Genotyping identifies the ~70% of patients who can be safely downgraded to clopidogrel to prevent major bleeding without sacrificing ischemic protection (POPULAR GENETICS).