ECG Challenge
Related Posts


About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal
8 Comments
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal
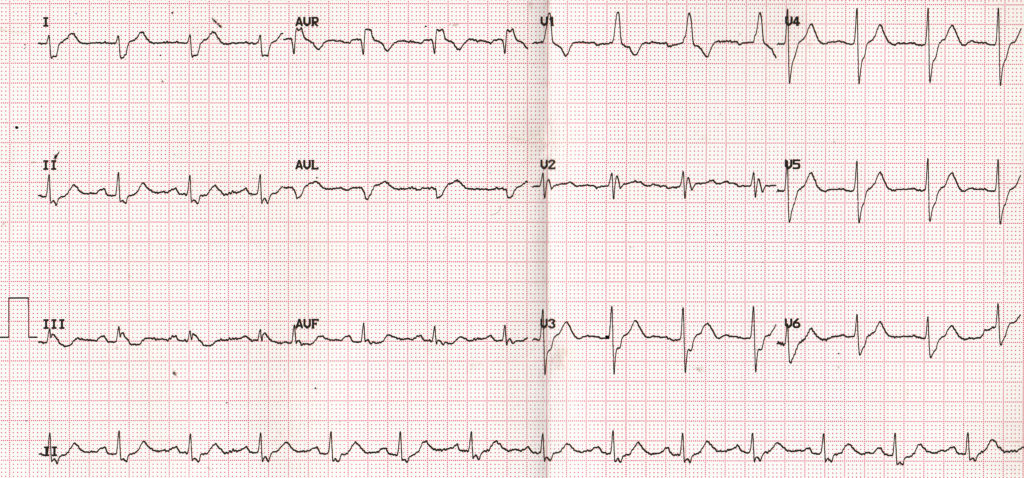
RBBB,RAD (NORTHWEST),LPFB
RAD
RVH
Incomplete RBBB
Subtle STE in lead 3
Possibilty of pulmonary embolism should be considered if it is acute in presentation
That was an instantaneous response! But North West axis should have QRS negative in lead I and aVF. Here the QRS is positive in aVF.
Why incomplete RBBB? QRS width is almost 160 ms – check for the widest QRS in standard leads.
Rvh
Rbbb
Right axis.
Right ventriculair strain pattern II,III and avf sadle brugada like pattern v2
Rvh
Rbbb
Right axis.
Borderline PR
rbbb..lpfb….rad…..bifascicular block
SR, RBBB, mean axis is rightward (pre-blocked frontal axis is normal). Of note is the monomorphic R-wave in V1, because with the normal pre-blocked axis I would expect at least an S-wave in V1. Perhaps that is lead positioning, prior posterior MI, or RVH.
On a cold read, all of the ST/T-waves appear reasonable. However, you can imagine relative ST-depression in III and ST-elevation in aVL, pointing towards a subtle high lateral infarction. I would not leave that off the list of possibilities, but couch that against the patient’s presentation.