



Electrolyte imbalances can profoundly affect the cardiac conduction system, leading to distinct patterns on an ECG. These changes are often the first clinical sign of life-threatening disturbances.
1. Potassium
Potassium is the most critical electrolyte regarding ECG changes because of its role in repolarization.
Hyperkalemia
As levels rise, the ECG typically progresses through these stages:
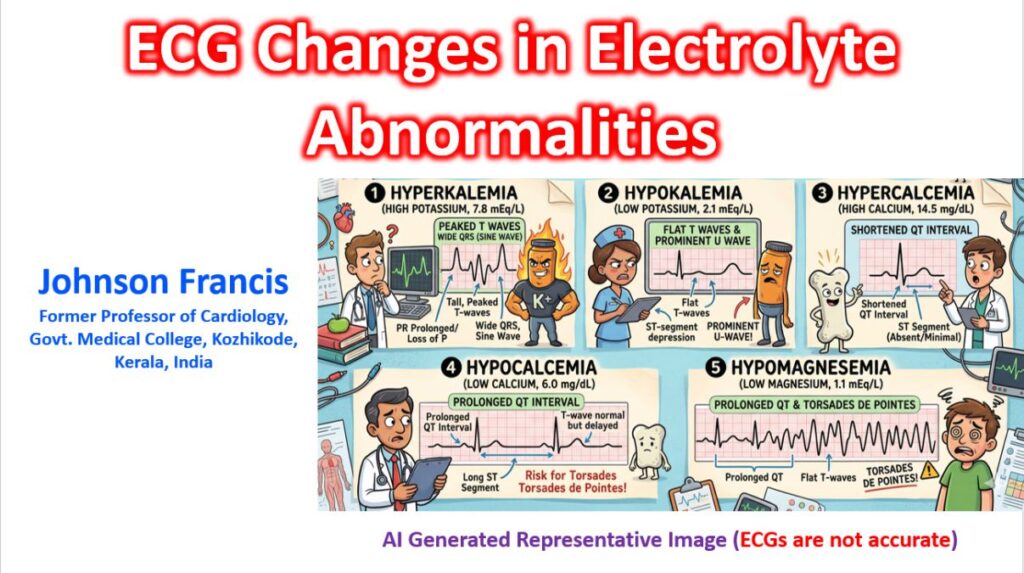
- Mild: Tall, “peaked” T-waves (narrow base, symmetrical).
- Moderate: P-wave flattens and eventually disappears; PR interval prolongs.
- Severe: QRS widens, merging with the T-wave to form a “sine wave” pattern. This is a precursor to ventricular fibrillation or asystole.
Hypokalemia
- Flattened T-waves and ST-segment depression.
- Prominent U-waves (seen after the T-wave, best in V2–V3).
- Prolonged QU interval (often mistaken for a long QT).
- Increased risk of tachyarrhythmias like Torsades de Pointes.
2. Calcium
Calcium primarily affects the duration of the ST segment rather than the morphology of the waves themselves.
Hypercalcemia
- Shortened QT interval.
- The ST segment is nearly absent; the T-wave begins almost immediately after the QRS complex.
- In severe cases, J-waves may occasionally appear. Though Osborn described the wave named after him in hypothermia, there is also a view that all J waves can be called Osborn waves.
Hypocalcemia
- Prolonged QT interval (specifically due to a lengthened ST segment).
- The T-wave itself remains normal in shape, but it is “pushed” further away from the QRS.
- Can predispose a patient to Torsades de Pointes.
3. Magnesium
Magnesium abnormalities often coexist with potassium and calcium issues as it is the cofactor for the enzyme transporting those ions in the kidney.
- Hypomagnesemia: Commonly presents with a prolonged QT interval and flattened T-waves. Its most famous complication is Torsades de Pointes (polymorphic ventricular tachycardia).
- Hypermagnesemia: Rare (usually seen in renal failure). It causes bradycardia, PR prolongation, and QRS widening.