



Echocardiography is the first-line non-invasive imaging modality for evaluating suspected pulmonary arterial hypertension (PAH). While right heart catheterization (RHC) remains the gold standard for definitive diagnosis, an echocardiogram provides critical data on the structural impact, hemodynamic severity, and right ventricular (RV) function. Key echocardiographic findings in PAH are broken down into structural changes, hemodynamic markers, and indices of RV systolic function.
Structural Findings (2D & M-Mode)
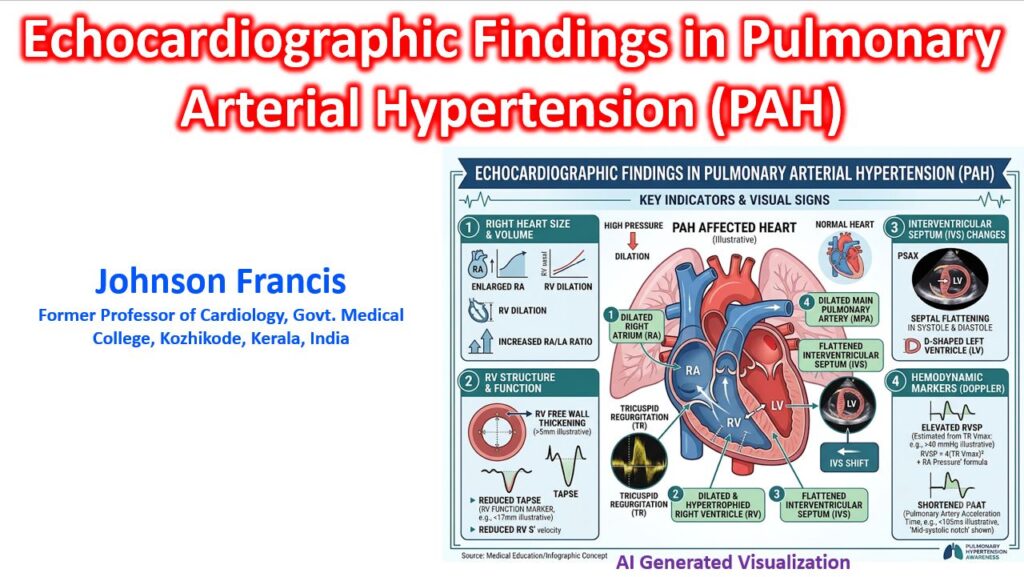
Chronic pressure and volume overload in PAH cause progressive right-sided remodeling, often at the expense of the left heart chambers.
- Right Ventricle (RV) Dilation: An RV basal diameter > 41 mm or an RV/LV basal diameter ratio > 1.0 in the apical 4-chamber view.
- RV Hypertrophy: Free wall thickness > 5 mm, measured in the subcostal view at end-diastole.
- Right Atrium (RA) Enlargement: End-systolic RA area > 18 cm², reflecting chronically elevated filling pressures.
- Pulmonary Artery (PA) Dilation: Main PA diameter > 25 mm.
- The “D-Shaped” Left Ventricle: A classic sign seen in the parasternal short-axis view. Increased right-sided pressures cause the interventricular septum to flatten or bow into the LV. In PAH, this flattening occurs in both systole and diastole (LV eccentricity index > 1.1), resulting in a D-shaped LV cavity.
Hemodynamic Markers (Doppler)
Doppler interrogation is essential for estimating pulmonary pressures and assessing the probability of PAH.
- Tricuspid Regurgitation Velocity (TRV): The primary metric used to estimate RV systolic pressure (RVSP). A peak TRV > 2.8 m/s suggests elevated pulmonary pressures.
- RVSP Calculation: Using the simplified Bernoulli equation, RVSP is estimated as
RVSP = 4(TRV)2 + RAP. - Inferior Vena Cava (IVC) Assessment: Used to estimate Right Atrial Pressure (RAP). An IVC > 21 mm that collapses less than 50% with inspiration indicates elevated RAP.
- Pulmonary Artery Acceleration Time (PAAT): Measured using pulsed-wave Doppler in the RV outflow tract. A shortened PAAT indicates increased pulmonary vascular resistance. A mid-systolic notch (corresponding “flying W” sign on M-Mode) in the Doppler envelope is highly specific for severe PAH.
- Pulmonary Regurgitation (PR): An early diastolic PR velocity > 2.2 m/s correlates with elevated mean pulmonary artery pressures.
Right Ventricular Function
Because RV failure drives mortality in PAH, assessing longitudinal and global RV contractility is crucial for prognosis.
| Metric | Threshold for Dysfunction | Clinical Significance |
| TAPSE | < 17 mm | Tricuspid Annular Plane Systolic Excursion measures longitudinal contraction. It is highly reproducible and strongly correlates with survival. |
| Tissue Doppler S’ | < 9.5 cm/s | The peak systolic velocity of the lateral tricuspid annulus. |
| RV FAC | < 35% | Fractional Area Change offers a 2D assessment of global RV systolic function. |
| TAPSE/sPAP Ratio | < 0.55 mm/mmHg | A marker of RV-PA coupling. It assesses whether the RV contractility (TAPSE) is adequately matched to the afterload (systolic pulmonary artery pressure). |
Clinical Note: The presence of a pericardial effusion is a significant, poor prognostic marker in PAH, indicating advanced right heart failure and elevated systemic venous pressures.