Prosthetic mitral valve echocardiogram
Prosthetic mitral valve echocardiogram
Evaluation of prosthetic valves is one of the difficult tasks in echocardiography because of the dense shadows caused by prosthetic valves. It may be virtually impossible to detect small lesions like a vegetation on the far side of the prosthetic valve. At the same time, a prosthetic valve endocarditis has a much more dismal prognosis than a native valve endocarditis. Moreover, even normally functioning prosthetic valves may have a gradient across which would be considered abnormal for a native valve.
 Prosthetic mitral valve – systolic frame
Prosthetic mitral valve – systolic frame
Echocardiogram of prosthetic mitral valve in parasternal long axis view showing the valve in the closed position and the aortic valve in the open position. The metallic component of the prosthetic valve produces dense echoes. The left atrium is dilated, possibly a sequelae of the old lesion for which the mitral valve was replaced. The aorta is relatively small, and left ventricle is of normal size, indicating that the lesion could have been mitral stenosis. When a prosthetic valve is placed in a case of isolated mitral stenosis, especially one of the caged ball variety with a high profile, the cage will jut into the left ventricular outflow tract and may increase the LV outflow gradient. LV: left ventricle; LA: left atrium; Ao: aorta; Prosth MV: prosthetic mitral valve.
 Prosthetic mitral valve – with valve in open position
Prosthetic mitral valve – with valve in open position
This picture shows the prosthetic mitral valve in the open position. See the dense acoustic shadowing behind the valve, which obviously can obscure small vegetations in that region. Getting a transesophageal echo is a way to look at the far side of the prosthetic valve when an endocarditis is suspected clinically. In transesophageal echocardiography, since the transducer is behind the left atrium the atrial aspect of the prosthetic valve can be imaged without interference by acoustic shadowing.
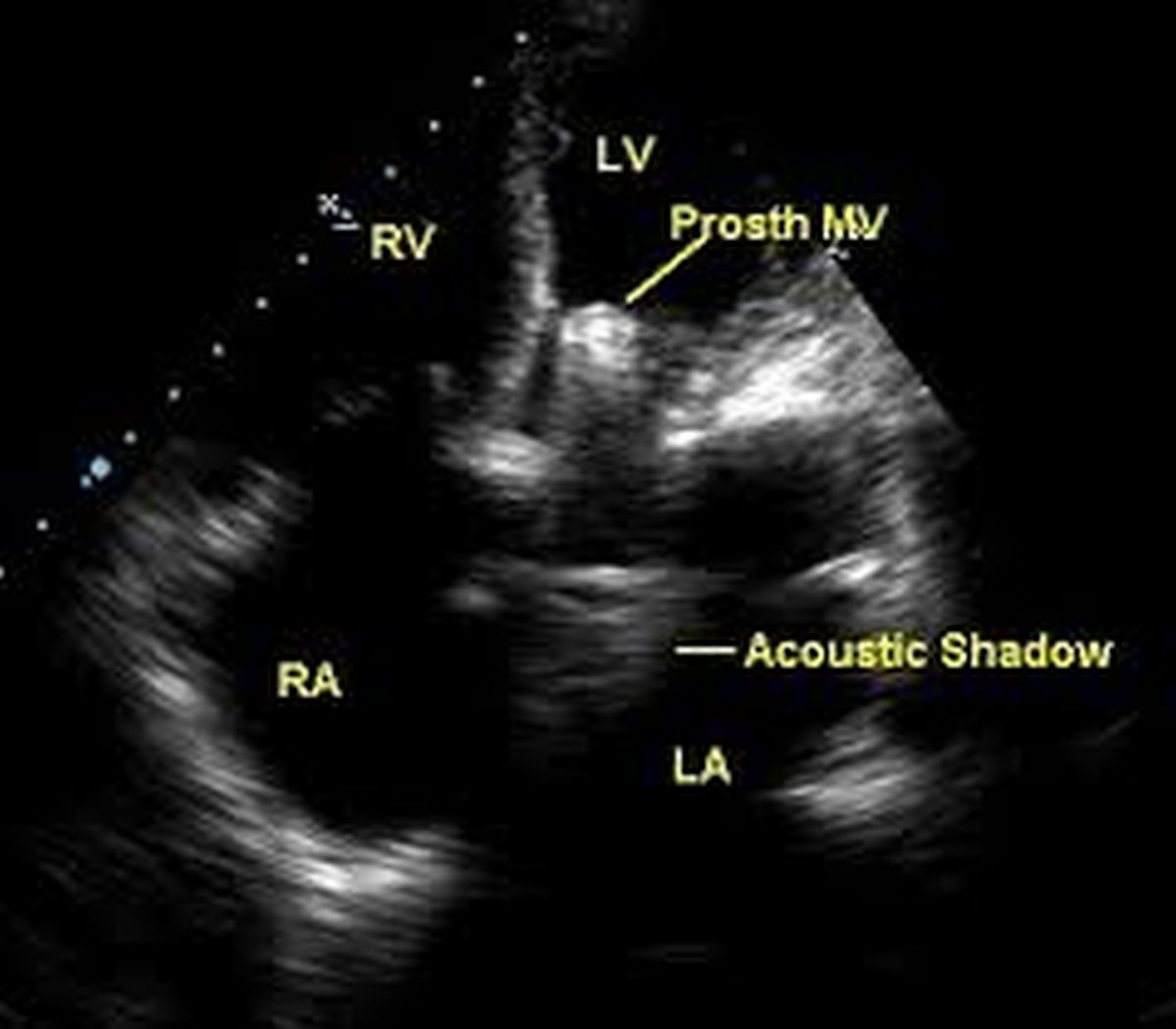 Prosthetic mitral valve in apical four chamber view
Prosthetic mitral valve in apical four chamber view
Apical four chamber view is also useful in the evaluation of the prosthetic mitral valve. Acoustic shadowing is a problem in this view also. RA: right atrium; RV: right ventricle
An M-mode cut of the prosthetic mitral valve is useful in documenting the poppet excursion. Poppet excursion is diminished in case of thrombus or pannus formation. Thrombus formation usually presents with acute mitral valve obstruction while pannus formation presents more insidiously with increasing gradients and effort intolerance.
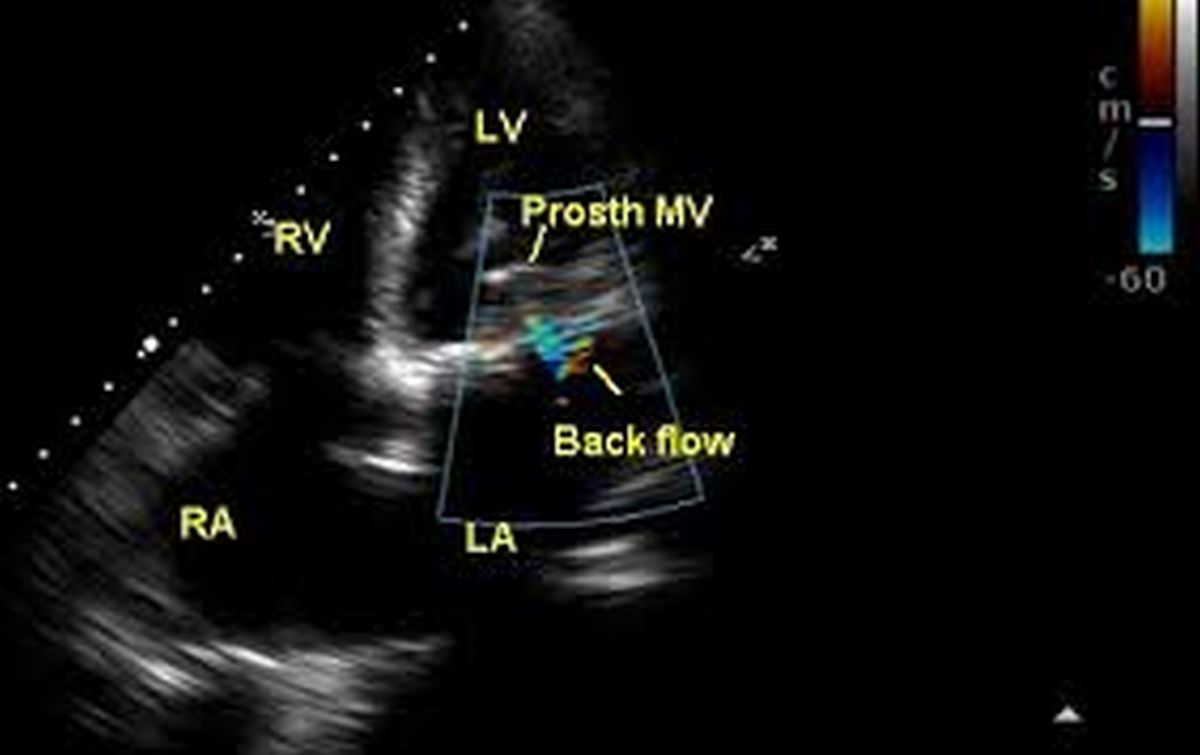 Prosthetic mitral valve in apical four chamber view with colour flow mapping
Prosthetic mitral valve in apical four chamber view with colour flow mapping
Colour flow mapping (color Doppler) from the apical four chamber view shows normal antegrade flow and a trivial backflow, which is normal during the closing movement of the prosthetic valve. This view is useful to look for para valvar and trans valvar leaks. Early onset of paravalvar leak may indicate the give way of a surgical suture. Doppler interrogation from this view is useful in quantifying the transvalvar gradients. It is always good to document the gradients serially to identify rise in gradients due to pannus formation. Acute obstruction usually presents with pulmonary edema due to grossly elevated pulmonary venous pressures and calls for urgent intervention.
Related Posts

About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal