



Fractional Flow Reserve (FFR) is the current gold standard for the physiological assessment of coronary artery stenosis. It is defined as the ratio of maximum blood flow in a stenotic artery to the maximum blood flow in the same artery if it were normal.
I. Technical Procedure & Protocols
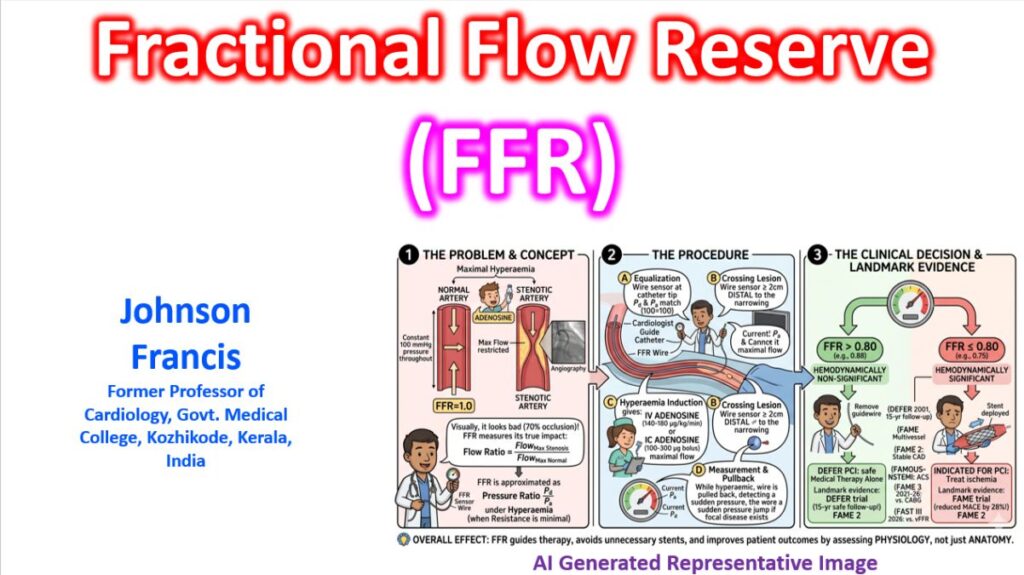
The FFR technique measures the pressure gradient across a lesion during maximal hyperaemia, where resistance is minimal and constant. At this state, the pressure ratio (Pd/Pa) directly reflects the flow ratio.
1. Procedure Steps
- Anticoagulation & Nitrates: Intravenous heparin and intracoronary (IC) nitroglycerin are administered to prevent thrombus and vasospasm.
- Equalization (Normalization): The pressure wire sensor is placed at the tip of the guiding catheter. Pressures from the wire (Pd) and the catheter (Pa) must be identical before advancing.
- Crossing the Lesion: The wire is advanced at least 2 cm distal to the stenosis.
- Induction of Hyperaemia:
- Intravenous (IV) Adenosine: Given via a large peripheral or central vein. OR
- Intracoronary (IC) Adenosine: A bolus of adenosine, with dose changing between right and left coronary artery provides rapid, well-tolerated hyperaemia.
- Pullback Technique: Under continuous hyperaemia, the wire is slowly withdrawn. A sudden “jump” in pressure identifies the specific focal lesion responsible for the gradient, whereas a gradual rise suggests diffuse disease.
- Drift Check: After the procedure, the sensor is returned to the catheter tip to ensure Pd and Pa still match, ruling out technical “pressure drift.”
2. Interpretation
- FFR > 0.80: Hemodynamically non-significant; revascularization can safely be deferred.
- FFR ≤ 0.80: Significant ischemia; revascularization (PCI/CABG) is generally indicated.
II. The Evidence Base: Landmark Trials
The transition from “oculostenotic” (visual) to “physiologic” (functional) guided intervention is supported by several decades of randomized controlled trials (RCTs).
DEFER (2001)
Deferring PCI for lesions with FFR > 0.75 in stable CAD is safe; 15-year data shows lower myocardial infarction risk in the deferred group (2.2% vs 10.0%), suggesting that stenting non-ischemic lesions may actually increase the risk of late events. The study had enrolled 325 patients scheduled for PCI of an intermediate stenosis. FFR was measured just before the planned intervention. If FFR was ≥0.75, patients were randomly assigned to deferral which had 91 patients or to PCI group, which had 90 patients. Long term follow up shows that there is no ‘catch-up’ phenomenon. There was no significant difference in mortality rates between the two groups at 15 years (33% vs 31%).
FAME (2009)
Study had 1005 patients from United States and Europe. Patients with multivessel disease, assigned to angiography-guided PCI group underwent stenting of all indicated lesions, whereas those assigned to FFR-guided PCI group underwent stenting of indicated lesions only if the FFR was 0.80 or less. Primary end point evaluated in the study was the rate of death, nonfatal myocardial infarction, and repeat revascularization at 1 year. In multivessel disease, FFR-guided PCI reduced event rate by 28% at 1 year compared to angiography-guided PCI (18.3% vs 13.2%).
FAME 2 (2012)
Patients in whom at least one stenosis was functionally significant with FFR, ≤0.80 were randomly assigned to FFR-guided PCI plus the best available medical therapy or the best available medical therapy alone. FFR-guided PCI significantly reduced the need for urgent revascularization compared to medical therapy alone. Recruitment was halted prematurely because of a significant between-group difference in the percentage of patients who had a primary end-point event: 4.3% in the PCI group and 12.7% in the medical-therapy group.
FAMOUS–NSTEMI (2015)
FFR-guided management in ACS changed treatment strategy in 22% of cases and reduced unnecessary PCI. That was a prospective, multicentre, parallel group, 1 : 1 randomized, controlled trial in 350 NSTEMI patients with ≥1 coronary stenosis ≥30% of the lumen diameter assessed visually, which was the threshold for FFR measurement. Fractional flow reserve was disclosed to the operator in the FFR-guided group which had 176 patients. FFR was measured but not disclosed in the angiography-guided group which comprised of 174 patients. FFR ≤0.80 was an indication for revascularization by PCI or CABG. At one year, revascularization remained lower in the FFR-guided group, 79.0 vs. 86.8%. There were no statistically significant differences in health outcomes and quality of life between the groups.
FAME 3 (2025)
FAME 3 was a multicentre, randomised trial comparing FFR-guided PCI using current-generation zotarolimus-eluting stents versus CABG in patients with three-vessel CAD not involving the left main coronary artery. 1500 patients with no cardiogenic shock, no recent STEMI, no severe LV dysfunction, and no previous CABG were randomized. At the 5-year follow-up, there was no significant difference in a composite outcome of death, stroke, or myocardial infarction after FFR-guided PCI versus CABG. But myocardial infarction and repeat revascularisation were higher in the PCI group.
FAST III (2026)
Angiography-derived vFFR (wire-free) was non-inferior to traditional wire-based FFR at 1 year. This was an international, open-label, randomized, noninferiority trial conducted across at 37 sites in Europe. Patients had coronary diameter stenosis from 30 – 80% and had presented with chronic or acute coronary syndromes. Primary endpoint was composite of death from any cause, any myocardial infarction or any revascularization at 1 year. Non Inferiority margin was taken as 3.0 percentage points. Vessel (or Virtual) fractional flow reserve (vFFR) was derived from three-dimensional quantitative coronary angiography without the need for a pressure wire or hyperemic agent.