


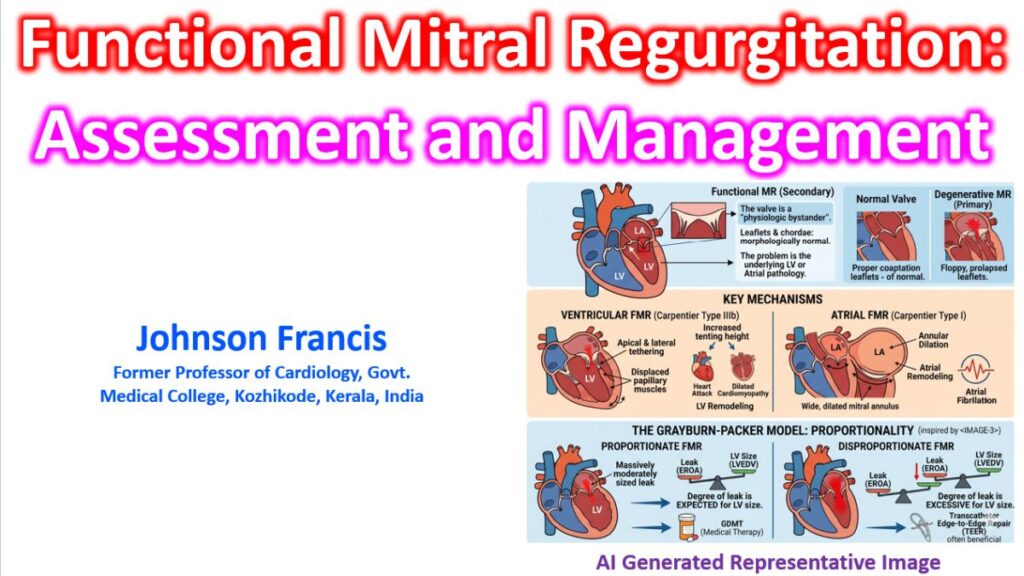

Functional Mitral Regurgitation (FMR), or secondary MR, represents a complex interplay where the mitral valve is a “physiologic bystander” to underlying left ventricular (LV) or atrial pathology. Unlike primary MR, the leaflets and chordae are typically morphologically normal; the regurgitation arises from geometric changes that prevent proper coaptation.
Pathophysiology and Classification
FMR is most commonly classified using the Carpentier system as Type IIIb (restricted motion during systole) or Type I (annular dilation).
- Ventricular FMR: LV remodeling—often from ischemic heart disease or dilated cardiomyopathy—leads to papillary muscle displacement. This results in apical and lateral tethering of the leaflets, increased tenting height, and tenting area.
- Atrial FMR: Increasingly recognized in patients with chronic atrial fibrillation. Massive annular dilation and impaired annular dynamics prevent the leaflets from meeting, even in the absence of significant LV dysfunction.
The Assessment Dilemma: EROA Thresholds
One of the most debated aspects of FMR was the threshold for “severity.” The discrepancy between guidelines historically centered on the Effective Regurgitant Orifice Area (EROA).
- One set: Generally utilizes a threshold of ≥ 0.4 cm2 for severe MR (harmonized with primary MR).
- Other set: Previously utilized≥ 0.2 cm2 as severe, arguing that lower volumes carry higher prognostic risk in heart failure patients.
Proportionate vs. Disproportionate FMR
The Grayburn-Packer model helps explain why some patients respond to transcatheter intervention while others do not:
- Proportionate FMR: The degree of MR is expected for the degree of LV dilation. These patients rarely benefit from edge-to-edge repair (TEER) as the primary problem is the ventricle.
- Disproportionate FMR: The MR is “excessive” relative to the LV end-diastolic volume (LVEDV). These patients (similar to the COAPT trial population) show significant mortality benefits from TEER.
Management Strategies
| Strategy | Clinical Context |
| GDMT | The cornerstone. ACEi/ARBs/ARNI, Beta-blockers, MRAs, and SGLT2 inhibitors can promote reverse remodeling and reduce FMR. |
| CRT | In patients with LBBB and wide QRS, Cardiac Resynchronization Therapy can improve papillary muscle coordination and reduce MR acutely. |
| TEER (MitraClip) | Indicated for symptomatic patients on optimal GDMT with “disproportionate” MR (EROA ≥ 0.3 cm2 and LVEDV < 70 ml/m2). |
| Surgery | Generally reserved for patients undergoing CABG/AVR. Isolated mitral surgery for FMR (undersized annuloplasty or replacement) has high recurrence rates and no proven survival benefit over medical therapy alone. |
Technical Indicators on Echocardiography
When evaluating for potential intervention, specific geometric measurements are critical:
- Tenting Height: The distance between the mitral annular plane and the coaptation point. A tenting height > 10 mm is a technical indicator of severe restriction and is associated with a high risk of annuloplasty failure.
- Tenting Area: The area enclosed by the leaflets and the annular plane in the apical four-chamber view. A tenting area > 2.5 cm² suggests significant leaflet tethering.
- Posterior Leaflet Angle (PLA): The angle between the posterior leaflet and the annular plane. A PLA > 45° is a strong predictor of recurrent MR after surgical ring annuloplasty.