

General examination – eyes and facial dysmorphism
Clinically examination is guided by the symptoms. Unless the history is not correlated with findings, important diagnostic possibilities may be missed. Clinical examination starts off with a focused general examination followed by a detailed examination of the cardiovascular system. Relevant points in other systems like basal crepitations, hepatosplenomegaly and neurological deficits should be looked for.
Examination strategy should be fitting to the clinical situation. When a patient presents to the emergency room, it should be a short but focused examination to permit early initiation of emergency management. Examination in the floor should be a detailed examination, unearthing all possible differential diagnoses to plan further investigations and management.
General Examination
General appearance of the person will give you an idea on whether emergency management is needed or not. Do not wait for detailed evaluation if the person is moribund. Start resuscitatory measures along with your assessment. General examination can proceed in a head to foot order so that important points are not missed.
Examination of eyes
As part of general examination, eyes have a lot of information in relation to cardiovascular disorders.
- Look for pallor, jaundice, cyanosis, and polycythemia. Last two are seen in congenital cyanotic heart disease.
- Squint with ocular muscle weakness, a feature of Kearns-Sayre syndrome may be associated with complete heart block.
- Hypertelorism and epicanthic folds are noted in Down syndrome.
- Cataract in congenital rubella syndrome with patent ductus arteriosus or peripheral pulmonary stenosis.
Facial dysmorphism
Epicanthic folds and ptosis also come under facial dysmorphism, along with down sloping palpebral fissures and can be seen in Noonan syndrome associated with pulmonary stenosis.
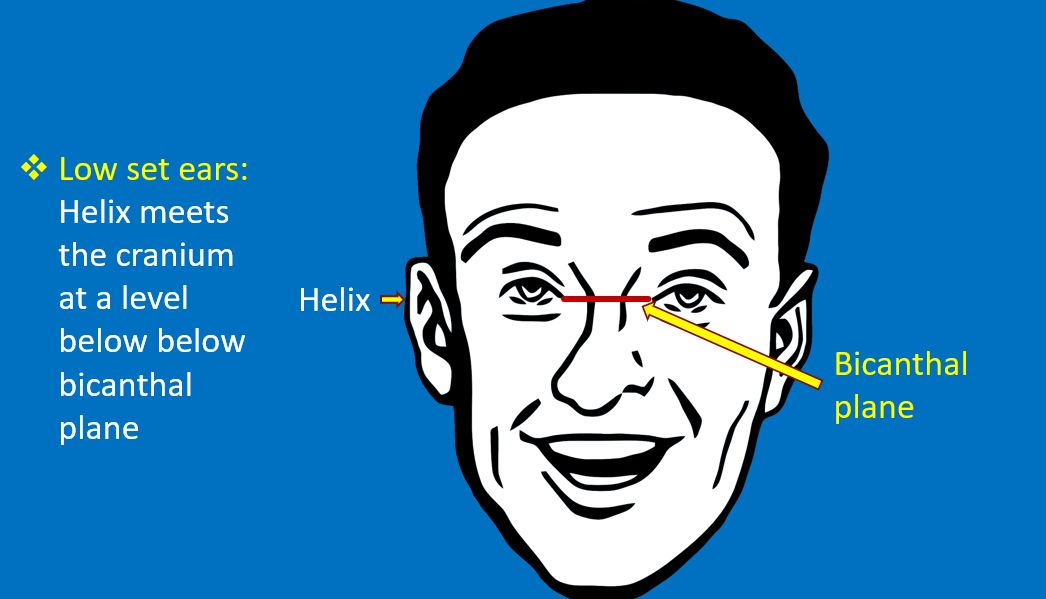
Low set ears can be seen in Noonan syndrome, Down syndrome and Di George syndrome. Latter two are associated with different types of cardiovascular defects.

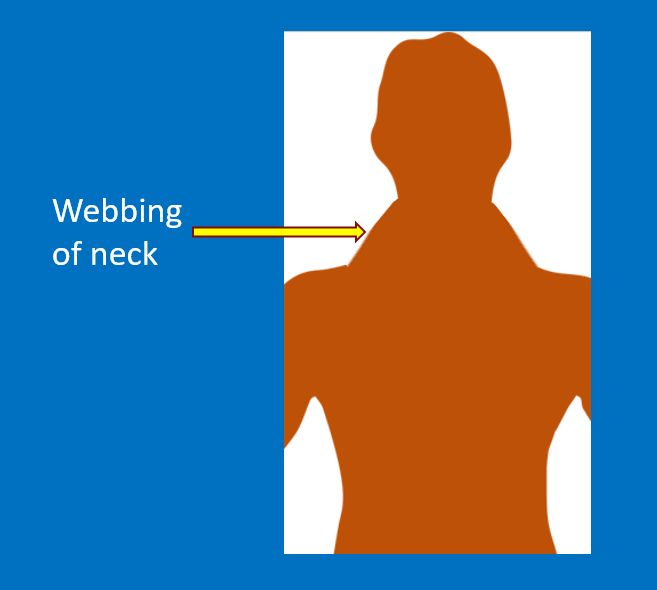
Webbing of neck is seen in Turner syndrome and Noonan syndrome (sometimes called male Turner syndrome though it occurs in both males and females). Turner syndrome is associated with coarctation of aorta.

Cleft lip and palate have been associated with multiple types of cardiac defects including ventricular septal defect, tetralogy of Fallot and tricuspid atresia.
Facial dysmorphism is also a feature in Andersen-Tawil syndrome, a type of long QT syndrome with inherited arrhythmias and periodic paralysis.
High arched palate is a feature in Ehlers-Danlos Syndrome and Marfan syndrome. Both can be associated aortic root dilatation and aortic regurgitation.