



The hemodynamics of constrictive pericarditis (CP) are defined by a rigid, noncompliant pericardium that encases the heart, leading to a “fixed” total cardiac volume. This pathological state results in two primary hemodynamic hallmarks: the dissociation of intrathoracic and intracardiac pressures and exaggerated ventricular interdependence.
1. Core Pathophysiological Hallmarks
The rigid pericardial shell insulates the heart from the normal pressure fluctuations of the respiratory cycle.
- Dissociation of Pressures: In a healthy heart, the inspiratory drop in intrathoracic pressure is transmitted to the heart chambers, facilitating venous return. In CP, the thickened pericardium prevents this transmission. Consequently, the pressure gradient for filling the left atrium (pulmonary capillary wedge pressure minus left atrial pressure) decreases during inspiration, leading to reduced left-sided filling.
- Enhanced Ventricular Interdependence: Because the total volume within the pericardium is fixed, the ventricles must compete for space. As the right ventricle (RV) fills more during inspiration (due to increased systemic venous return), the interventricular septum is pushed toward the left, further reducing left ventricular (LV) filling and stroke volume.
2. Invasive Hemodynamic Findings
Cardiac catheterization remains a definitive method for identifying the specific “constrictive” profile.
| Finding | Description | Mechanism |
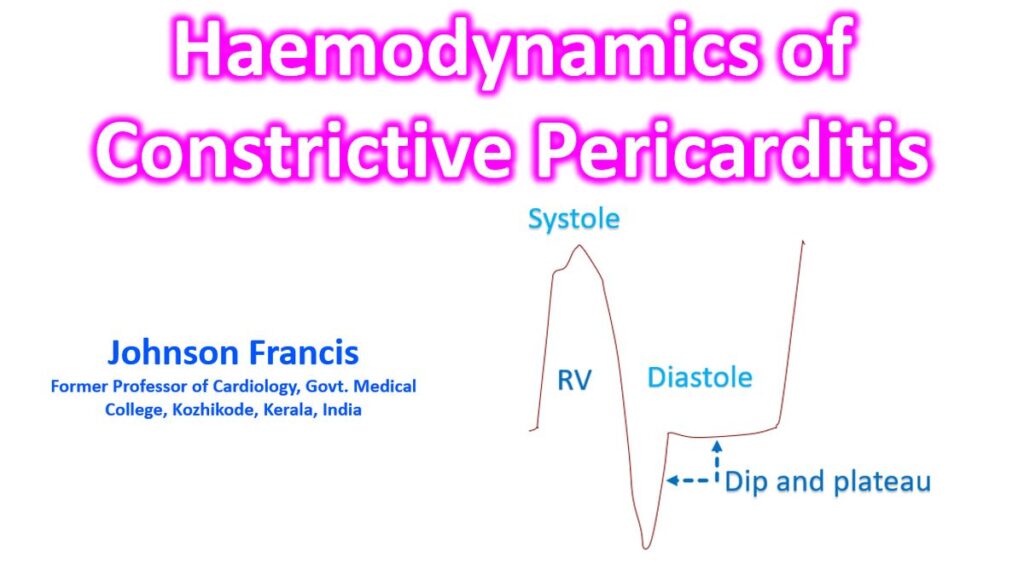
| Square Root Sign | A rapid early diastolic “dip” followed by a flat “plateau.” | Fast early filling that halts abruptly when the rigid pericardium is reached. |
| Equalization of Pressures | Diastolic pressures in all four chambers equalize (within 5 mmHg). | The rigid shell dictates a common filling pressure for the entire heart during diastole. |
| Prominent Y-Descent | A sharp, deep drop in atrial/venous pressure at the start of diastole. | Reflects the rapid, unimpeded early filling of the ventricles before the pericardial limit is hit. |
| Kussmaul’s Sign | A paradoxical rise (or lack of fall) in jugular venous pressure (JVP) during inspiration. | The RV cannot accommodate the inspiratory increase in venous return due to the noncompliant shell. |
3. Respirophasic Dynamics: The Key Differentiator
The most critical diagnostic finding in the cath lab is ventricular discordance, which helps distinguish CP from restrictive cardiomyopathy (RCM).
- Ventricular Discordance (CP): During inspiration, the RV systolic pressure increases while the LV systolic pressure decreases. They move in opposite directions (discordant).
- Ventricular Concordance (RCM): In restrictive disease, the RV and LV systolic pressures typically rise and fall together (concordant) because they are both subjected to the same intrathoracic pressure changes.
4. Non-Invasive Correlates
Modern imaging translates these hemodynamics into visual markers:
- Echocardiography: Features include the “septal bounce“ (an abrupt shift of the septum toward the LV in early diastole) and “annulus reversus“ (where the medial mitral annular velocity e’ is higher than the lateral velocity, reversing the normal pattern).
- Cardiac MRI/CT: Useful for visualizing pericardial thickening (>3 mm) or calcification and assessing respirophasic septal shift via real-time “cine” sequences.
References
- Khraishah H, Kwun A, Dearani JA, Alfaddagh A. Constrictive Pericarditis: A Comprehensive Overview. Heart Views. 2025 Jul-Sep;26(3):188-197. doi: 10.4103/heartviews.heartviews_52_25. Epub 2025 Nov 21. PMID: 41393823; PMCID: PMC12697754.
- StatPearls. (2026). Constrictive Pericarditis. NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK459314/
- Doshi S, Ramakrishnan S, Gupta SK. Invasive hemodynamics of constrictive pericarditis. Indian Heart J. 2015 Mar-Apr;67(2):175-82. doi: 10.1016/j.ihj.2015.04.011. Epub 2015 May 13. PMID: 26071303; PMCID: PMC4475854.