


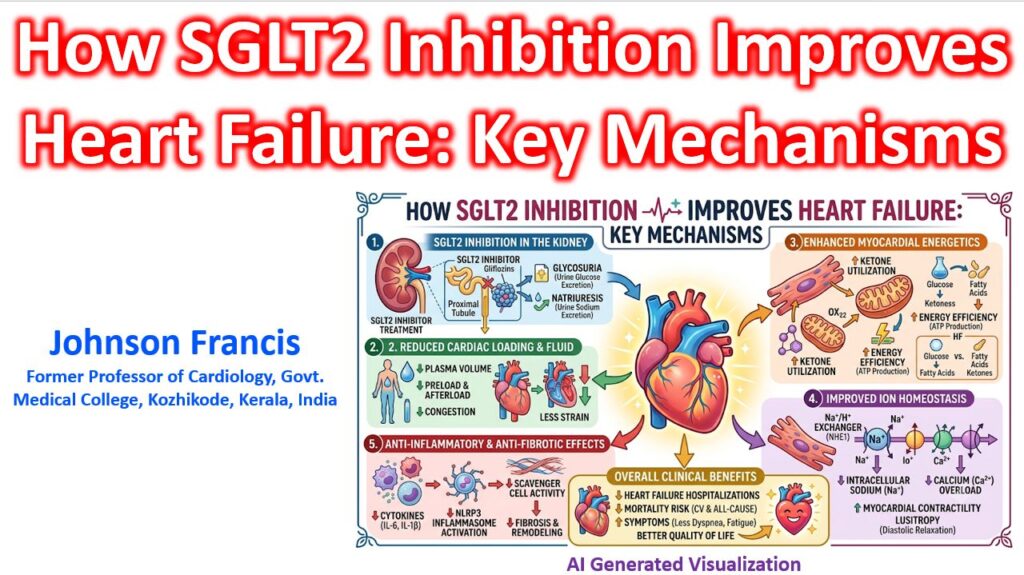

The cardioprotective benefits of SGLT2 inhibitors (like empagliflozin and dapagliflozin) have fundamentally shifted heart failure management. While initially designed for glycemic control, their profound efficacy in both HFrEF and HFpEF operates largely independently of insulin or glucose lowering. Instead, they act through a cascade of pleiotropic mechanisms that fundamentally alter cardiac loading, myocardial metabolism, and intracellular ion handling.
1. Hemodynamics and “Smart” Diuresis
SGLT2 inhibitors promote glycosuria and natriuresis at the proximal convoluted tubule, but their diuretic profile is functionally distinct from traditional loop diuretics. They preferentially reduce interstitial fluid volume rather than intravascular plasma volume. This decongests the tissues without causing the severe hemoconcentration or organ hypoperfusion that triggers neurohormonal rebound.
Furthermore, by blocking sodium reabsorption early in the nephron, they increase Na+ delivery to the macula densa. This restores tubuloglomerular feedback, actively suppressing the Renin-Angiotensin-Aldosterone System (RAAS) rather than stimulating it.
| Feature | SGLT2 Inhibitors | Loop Diuretics |
| Fluid Compartment Target | Interstitial fluid (decongestion) | Intravascular plasma |
| Neurohormonal Impact | Minimal to no SNS/RAAS activation | Significant reflex activation |
| Macula Densa Na+ | Increased (inhibits renin) | Decreased (stimulates renin) |
2. Myocardial Energetics (The “Thrifty Substrate” Hypothesis)
The failing heart is notoriously energy-starved. It pathologically shifts away from efficient free fatty acid oxidation toward inefficient glycolysis.
SGLT2 inhibitors induce a state of mild fasting mimicry, shifting whole-body metabolism to produce ketone bodies. The myocardium eagerly takes up β-hydroxybutyrate, a highly efficient “superfuel.” Oxidizing ketones yields significantly more ATP per molecule of oxygen consumed compared to fatty acids or glucose, directly improving mitochondrial efficiency and cardiac contractility without increasing oxygen demand.
3. Intracellular Ion Homeostasis (NHE1 Inhibition)
Despite low SGLT2 receptor expression in the myocardium, these drugs have direct, profound effects on cardiac tissue by inhibiting the Na+/H+ exchanger 1 (NHE1).
In heart failure, NHE1 is markedly overactive, pumping H+ out and Na+ into the cardiomyocyte. This intracellular sodium overload drives the reverse mode of the Na+/Ca2+ exchanger, pulling calcium into the cell.
- The Cost of Calcium Overload: Impaired diastolic relaxation (lusitropy), increased arrhythmogenesis, and the triggering of autosis (autophagic cell death).
- The SGLT2i Fix: By directly inhibiting NHE1, SGLT2 inhibitors lower intracellular Na+, preventing downstream calcium overload. This is a primary driver of their massive benefit in HFpEF, where diastolic stiffness is the core pathology.
4. Kidney-Heart Crosstalk and Inflammation
By blocking active transport in the proximal tubule, SGLT2 inhibitors significantly reduce the metabolic workload and oxygen demand of the kidneys. This reduction in tubulointerstitial hypoxia lowers afferent sympathetic nerve signaling from the kidney back to the heart.
Additionally, this improved renal microenvironment restores normal erythropoietin (EPO) production. The resulting mild increase in hematocrit improves oxygen delivery directly to the ischemic or failing myocardium. Finally, they actively suppress the NLRP3 inflammasome, blunting the systemic inflammation and subsequent myocardial fibrosis that drives adverse cardiac remodeling.