



Lead aVR has historically been dubbed the “forgotten lead” in electrocardiography. Because it looks at the heart from the right shoulder, all major depolarization vectors move away from it. In a normal heart, this typically results in a globally negative complex (inverted P wave, downward QRS, and inverted T wave). However, dismissing aVR as simply a “negative lead” is a missed diagnostic opportunity. It serves as a unique anatomical window into the basal septum, the right ventricular outflow tract, and the left main coronary artery.
Here is a breakdown of the critical clinical utilities of Lead aVR:
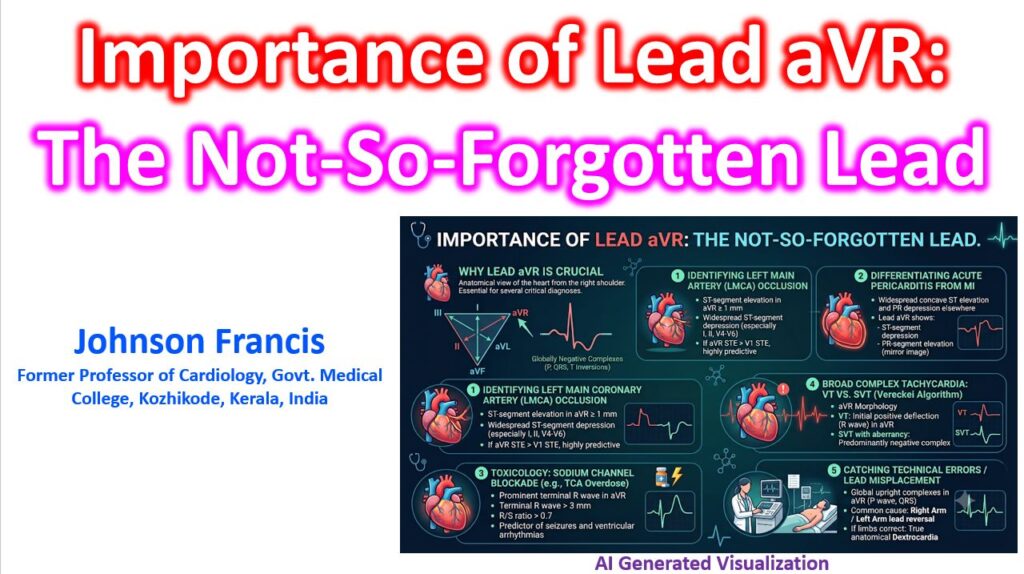
1. Identifying Left Main Coronary Artery (LMCA) Occlusion
This is perhaps the most life-saving application of aVR. In the setting of an acute coronary syndrome, severe ischemia to the basal septum can project directly toward the right shoulder.
- The Pattern: Widespread ST-segment depression in multiple leads (especially I, II, V4-V6) coupled with ST-segment elevation in aVR of 1 mm or more.
- Significance: If the ST elevation in aVR is greater than the ST elevation in lead V1, it is highly predictive of Left Main Coronary Artery (LMCA) occlusion or severe, proximal triple-vessel disease. This finding often warrants urgent angiography.
2. Differentiating Acute Pericarditis from Myocardial Infarction
Because of its unique axis, lead aVR acts as the reciprocal lead to the inferolateral leads (I, II, aVL, V4-V6).
- The Pattern: While acute pericarditis presents with widespread, diffuse concave ST-segment elevation and PR-segment depression, aVR will show the exact opposite: ST-segment depression and PR-segment elevation.
- Significance: A prominent elevated PR segment in aVR (mirroring the PR depression seen globally) is a classic, highly reliable hallmark of acute pericarditis.
3. Toxicology: Sodium Channel Blockade
Lead aVR is an essential screening tool for toxicological emergencies, specifically overdoses involving Tricyclic Antidepressants (TCAs) or other sodium channel blocking agents.
- The Pattern: A prominent terminal R wave in aVR.
- Significance: A terminal R wave greater than 3 mm, or an R/S ratio greater than 0.7 in aVR, strongly correlates with severe toxicity. It is a vital predictor of impending seizures and ventricular arrhythmias.
4. Broad Complex Tachycardia: VT vs. SVT
The Vereckei algorithm relies entirely on the morphology of lead aVR to differentiate Ventricular Tachycardia (VT) from Supraventricular Tachycardia (SVT) with aberrant conduction.
- Significance: Because SVT impulses travel down the normal His-Purkinje system (moving away from the right shoulder), aVR should be predominantly negative. If the initial deflection in aVR is positive (an initial R wave), it strongly suggests the electrical impulse is originating from the ventricles and moving upwards towards the atria, diagnosing VT.
5. Catching Technical Errors (Lead Misplacement)
Before interpreting the rhythm or ischemic changes, aVR serves as the ultimate quality-control check.
- Significance: If the P wave and QRS complex are globally upright in aVR, the most common cause is a Right Arm / Left Arm lead reversal by the technician. If you confirm the limb leads are placed correctly and aVR is still completely positive, it is a strong indicator of true anatomical dextrocardia.