



The electrical activity of the heart, which governs every heartbeat, is a finely tuned symphony of ions moving across cell membranes. These movements occur through specialized protein pores called ion channels. Understanding these channels is essential for grasping how the cardiac action potential works and how various anti-arrhythmic drugs exert their effects.
1. Sodium Channels (Na+)
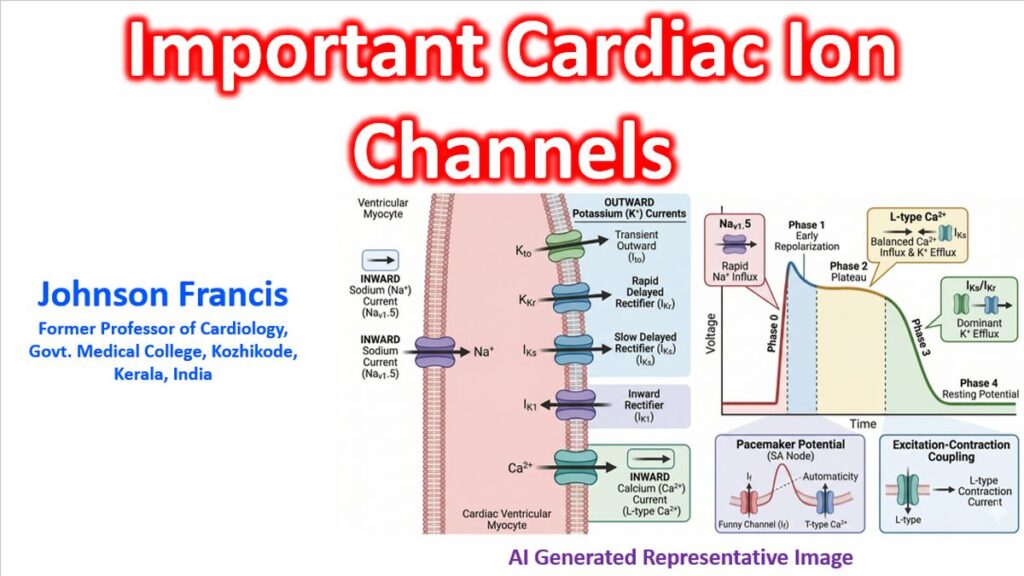
Sodium channels are responsible for the rapid “upstroke” of the action potential in non-pacemaker cells (atrial and ventricular myocytes).
- Primary Channel: Nav1.5 (encoded by the SCN5A gene).
- Function: They open rapidly in response to depolarization, allowing a massive influx of Na+ ions. This causes Phase 0 of the action potential.
- Clinical Significance: * Brugada Syndrome: Often caused by mutations in SCN5A.
- Class I Anti-arrhythmics: Drugs like Lidocaine or Flecainide work by blocking these channels.
2. Calcium Channels (Ca2+)
Calcium channels bridge the gap between electrical excitation and mechanical contraction (excitation-contraction coupling).
- L-type Calcium Channels (ICa,L): These are the “Long-lasting” channels. They open during Phase 2 (The Plateau Phase), allowing Ca2+ to enter the cell, which triggers the release of even more calcium from the sarcoplasmic reticulum to make the heart muscle contract.
- T-type Calcium Channels (ICa,T): “Transient” channels that play a larger role in the pacemaker activity of the SA and AV nodes.
- Clinical Significance: Calcium channel blockers (like Verapamil or Diltiazem) are used to control heart rate and treat hypertension.
3. Potassium Channels (K+)
Potassium channels are the “reset” buttons of the heart. They allow K+ to leave the cell, making the interior more negative again (repolarization).
Rapid and Slow Delayed Rectifier Channels (IKr and IKs)
- Function: These are responsible for Phase 3 repolarization, bringing the cell back to its resting state.
- Clinical Significance: * Long QT Syndrome: Mutations in these channels (like KCNH2 for IKr or KCNQ1 for IKs) delay repolarization, lengthening the QT interval and increasing the risk of Torsades de Pointes.
- Class III Anti-arrhythmics: Amiodarone and Sotalol primarily target these channels.
Inward Rectifier Channels (IK1)
- Function: These maintain the stable resting membrane potential during Phase 4.
4. The “Funny” Channel (If)
Found primarily in the pacemaker cells of the SA node, this channel is unique because it is activated by hyperpolarization (when the cell voltage gets low) rather than depolarization.
- Function: It allows a mixed current of Na+ and K+ to leak into the cell, causing a slow upward drift in voltage during Phase 4. This is what allows the heart to beat automatically without an external trigger.
- Clinical Significance: The drug Ivabradine selectively blocks this channel to slow the heart rate without affecting contractility.
Summary of Ion Movements
| Phase | Description | Primary Ion Movement | Channel Type |
| Phase 0 | Depolarization | Na+ Influx | Fast Na+ Channels |
| Phase 1 | Early Repolarization | K+ Efflux | Transient Outward K+ |
| Phase 2 | Plateau | Ca2+ Influx / K+ Efflux | L-type Ca2+ Channels |
| Phase 3 | Repolarization | K+ Efflux | Delayed Rectifier K+ |
| Phase 4 | Resting/Pacemaker | Na+/K+ Leak (If) | Funny Channels / IK1 |