


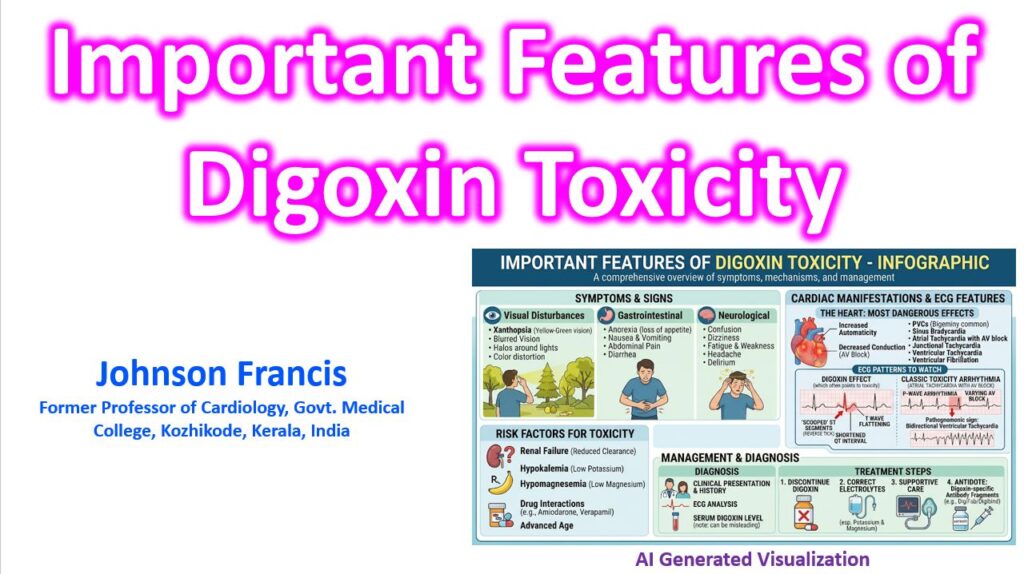

Here are the hallmark features of digoxin toxicity, focusing on the clinical presentation, electrolyte shifts, and the classic ECG findings.
1. ECG Manifestations
Digoxin toxicity creates a dangerous combination of increased automaticity (due to intracellular calcium overload) and decreased AV conduction (due to increased vagal tone).
- Most Common Arrhythmia: Premature Ventricular Contractions (PVCs).
- Most Specific Arrhythmias:
- Bidirectional Ventricular Tachycardia: Highly specific; alternates QRS axis beat-to-beat.
- Atrial Tachycardia with AV Block: The combination of ectopic atrial firing and AV nodal suppression is a classic hallmark.
- Other Rhythms: Junctional tachycardia, slow atrial fibrillation, and varying degrees of AV block.
Key Distinction: “Digoxin Effect” vs. Toxicity
Therapeutic levels produce the “digoxin effect” on an ECG, which is not synonymous with toxicity. This includes the classic “scooped” ST-segment depression or mirror image correction mark sign and shortened QT interval.
2. Clinical Symptoms
Non-cardiac symptoms often precede arrhythmias and are frequently misattributed to other causes, especially in older adults with vague complaints.
- Gastrointestinal (Earliest): Anorexia, nausea, vomiting, and diffuse abdominal pain.
- Neurological: Lethargy, confusion, weakness, and delirium.
- Visual Disturbances: Blurred vision and xanthopsia (seeing yellow or green halos around objects, or a generalized yellow tint to vision).
3. The Electrolyte Dynamics
The relationship between potassium and digoxin is critical for diagnosis and management, as they compete for the same binding site on the Na⁺/K⁺-ATPase pump.
| Feature | Acute Toxicity | Chronic Toxicity |
| Typical Patient | Intentional overdose or accidental ingestion | Elderly patient on long-term therapy with declining renal clearance |
| Potassium Level | Hyperkalemia (prognostic indicator of mortality) | Hypokalemia (precipitates toxicity) |
| Mechanism | Massive Na⁺/K⁺ pump blockade pushes K⁺ extracellularly | Concomitant diuretic use depletes K⁺, leaving more pump binding sites open for digoxin |
| Symptom Onset | Rapid (GI symptoms prominent early) | Insidious (neurological and visual symptoms often prominent) |
Note: Hypomagnesemia and hypercalcemia also increase myocardial sensitivity to digoxin and can independently precipitate toxicity.
4. Management Priorities
- Discontinue the drug and stop any potassium-depleting diuretics.
- Correct electrolytes: Carefully replete potassium and magnesium in chronic cases. Avoid calcium administration for hyperkalemia if digoxin toxicity is suspected (historically thought to cause “stone heart,” though modern evidence is mixed, it remains a standard precaution).
- Digoxin-specific Fab fragments (Digibind): The definitive antidote. Indicated for life-threatening arrhythmias (e.g., VT, VF, high-degree AV block), hemodynamically significant bradycardia unresponsive to atropine, or serum potassium > 5.0 mEq/L in the setting of acute toxicity.