



The short answer is no, it is not entirely obsolete, but its role has significantly narrowed in contemporary clinical practice.
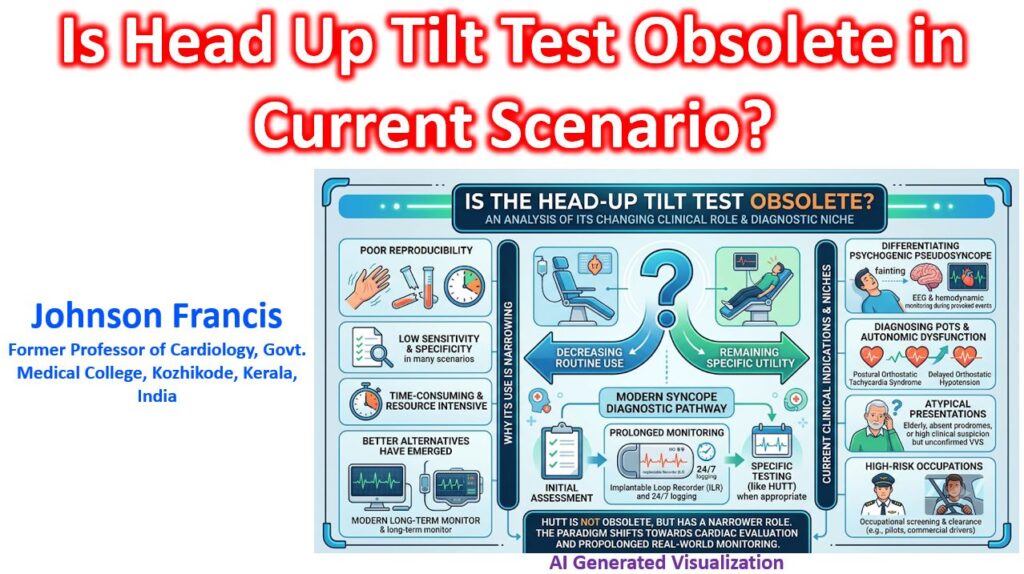
The Head-Up Tilt Test (HUTT) has transitioned from being a routine, first-line diagnostic tool for unexplained syncope to a highly specific, niche investigation. Its decline in routine use is largely due to its notoriously poor reproducibility, variable sensitivity and specificity, and the rise of more reliable long-term monitoring technologies.
Here is a breakdown of where HUTT stands in the current diagnostic landscape based on contemporary guidelines
Where HUTT is No Longer Recommended
- Classic Vasovagal Syncope (VVS): If the clinical history is classic for VVS (e.g., triggered by pain, standing, or emotion, with typical prodromes), diagnosing reflex syncope is clinical. A tilt test is redundant and unnecessary.
- Assessing Treatment Efficacy: HUTT is highly discouraged for evaluating whether a pharmacological therapy for VVS is working. The test lacks the reproducibility required to confidently determine if a negative second test is due to the drug or simply test variability.
- Unexplained Syncope with High Arrhythmic Risk: In patients with structural heart disease or abnormal baseline ECGs where an arrhythmic cause is strongly suspected, HUTT is bypassed in favor of electrophysiological studies (EPS) or prolonged monitoring.
The Current Clinical Niche (Where HUTT Still Adds Value)
Despite its limitations, HUTT remains a class IIa or IIb recommendation in specific, challenging scenarios:
- Differentiating Syncope from Psychogenic Pseudosyncope (PPS): This is currently one of the most valuable uses of the tilt test. In patients with frequent “swooning” or falls without true loss of consciousness, observing the patient during a provoked episode (often while recording video and concurrent EEG) can definitively diagnose PPS if hemodynamics remain perfectly stable during the event.
- Confirming Autonomic Failure: HUTT is highly useful for diagnosing delayed orthostatic hypotension (OH), postural orthostatic tachycardia syndrome (POTS), or unmasking underlying autonomic neuropathy (such as in Parkinson’s disease or multiple system atrophy) when active standing tests are borderline or inconclusive.
- Atypical Reflex Syncope: When a patient has unexplained syncope that is suspected to be reflex in nature but lacks the classic prodrome, HUTT can help confirm susceptibility to vasovagal reflexes. This is particularly relevant in older adults where the presentation might be atypical.
- Occupational/High-Risk Screening: For patients in high-risk professions (e.g., pilots, commercial drivers, heavy machinery operators), demonstrating a negative HUTT might be required for occupational clearance after an isolated, unexplained syncopal event.
The Shift to Prolonged Monitoring
The biggest driver rendering HUTT “less relevant” is the advent of the Implantable Loop Recorder (ILR) or Insertable Cardiac Monitor (ICM).
The paradigm has shifted from provoking an episode in an artificial lab setting to capturing the spontaneous clinical event in the real world. ILRs provide absolute symptom-rhythm correlation, which HUTT often fails to do. If a patient has recurrent, severe, unexplained syncope, modern pathways heavily favor early ILR implantation over an exhaustive, non-diagnostic autonomic testing battery.