



Ischemic mitral regurgitation (IMR) is one of the most challenging complications of coronary artery disease, shifting the clinical focus from a primary valve issue to a ventricular disease. It requires a nuanced, “lifetime management” strategy because the regurgitation is a dynamic consequence of adverse left ventricular (LV) remodeling rather than intrinsic structural leaflet disease.
Pathophysiology: The Tethering Problem
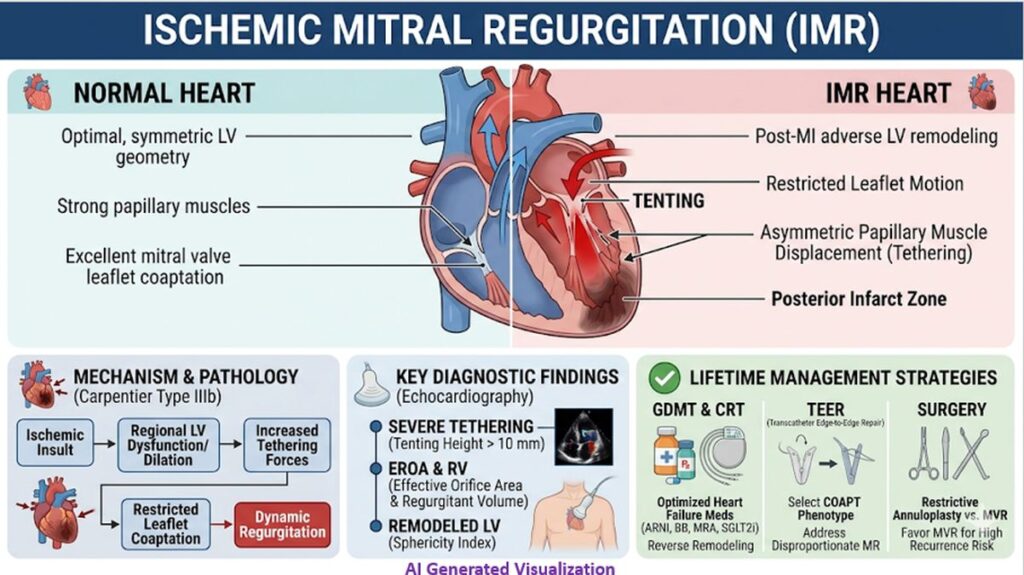
IMR is classically defined as a Carpentier Type IIIb dysfunction—restricted leaflet motion primarily during systole.
Acute or chronic ischemia (most commonly an inferior or posterior MI) leads to regional akinesis and adverse LV remodeling. This remodeling displaces the papillary muscles apically and laterally. The resulting imbalance between the closing forces (diminished by LV dysfunction) and the tethering forces (increased by papillary displacement) prevents adequate leaflet coaptation.
While annular dilatation occurs, the primary mechanical defect in IMR is this severe chordal tethering, often leading to the characteristic “tenting” of the leaflets.
Echocardiographic Hallmarks
Accurate assessment requires a multiparametric approach, as IMR is highly dynamic and sensitive to loading conditions.
- Tenting Parameters: A tenting height > 10 mm and a tenting area > 2.5 cm² are strong indicators of severe tethering and predict a higher risk of repair failure if surgical annuloplasty is attempted.
- Coaptation Depth: Abnormal coaptation depth reflects the severity of papillary displacement.
- Severity Thresholds: Historically, the threshold for severe secondary MR (EROA ≥ 20 mm², Regurgitant Volume ≥ 30 mL) was lower than for primary MR due to the poor prognosis associated with even moderate degrees of volume overload in an ischemic ventricle. The concept of proportionate vs. disproportionate MR is now essential when evaluating these parameters against the degree of LV dilatation.
Evolving Management Paradigms
The treatment landscape has shifted significantly over the last decade, moving away from a uniform surgical approach toward highly individualized strategies incorporating transcatheter options.
1. Guideline-Directed Medical Therapy (GDMT)
Maximal GDMT is the mandatory first step. Optimization with ARNI, beta-blockers, MRAs, and SGLT2 inhibitors promotes reverse LV remodeling. Cardiac Resynchronization Therapy (CRT) should be utilized if electrical dyssynchrony is present, as it can directly improve coordinated papillary muscle function and reduce MR severity.
2. Surgical Intervention (The CTSN Trials)
For patients undergoing CABG, addressing moderate or severe IMR simultaneously is common, but isolated surgery for IMR is controversial.
- Repair vs. Replacement: The CTSN trials demonstrated no significant difference in 2-year survival or LV reverse remodeling between undersized restrictive mitral annuloplasty and chordal-sparing mitral valve replacement. However, repair was associated with a significantly higher recurrence of moderate-to-severe MR (~32% vs. 2%). Consequently, for severe IMR with high-risk tethering parameters (e.g., severe basal aneurysm, tenting height > 11 mm), replacement is often favored over repair.
3. Transcatheter Edge-to-Edge Repair (TEER)
The contrasting results of the COAPT and MITRA-FR trials revolutionized patient selection for TEER (MitraClip) in secondary MR.
- The COAPT Phenotype (Disproportionate MR): Patients with severe MR (larger EROA) but without extreme LV dilatation derived a massive survival and symptomatic benefit from TEER. The MR in these patients was “disproportionately” severe relative to their LV dysfunction.
- The MITRA-FR Phenotype (Proportionate MR): Patients with massive LV dilatation where the MR was simply “proportionate” to the severely remodeled ventricle did not benefit from TEER; their primary issue was end-stage pump failure, not the volume overload of the valve.