Left main coronary artery disease on ECG
Left main coronary artery disease on ECG
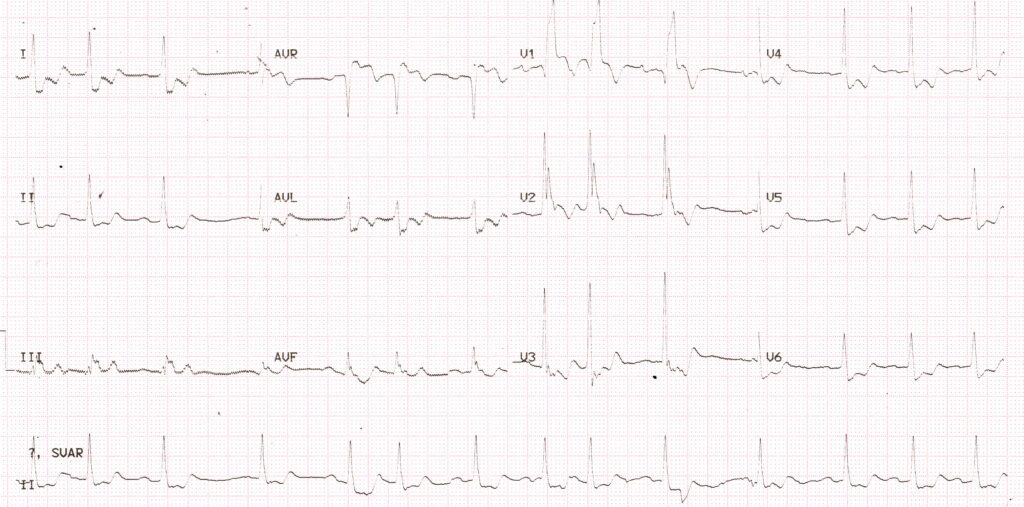
ST segment elevation in aVR and diffuse ST segment depression in inferior and anterolateral leads is considered a feature of significant left main coronary artery disease. The ECG shown above, there is ST segment elevation in aVR and V1 along with ST depression in inferior and lateral leads. ST elevation in aVR more than that in V1 is also suggestive of left main disease.
In a study comparing acute obstruction of left main, left anterior descending (LAD) and right coronary (RCA) occlusions, aVR ST elevation of more than 0.05 mV was noted in 88% of left main (LMCA) obstruction, 43% of LAD obstruction and 8% of RCA obstruction [1]. One limitation of the study was lack of comparison with left circumflex (LCX) obstruction.
In addition to ST elevation in aVR, this ECG also shows Q in V1 followed by a tall slurred R (QRBBB) is indicative of anterior wall infarction with right bundle branch block. The initial R of the RSR’ pattern expected in right bundle branch block (RBBB) is knocked off by the infarction. Multiple supraventricular ectopics are also seen in the ECG.
In a case reported by Shinde RS et al, coronary angiography documented total occlusion of left coronary artery and the patient underwent emergency coronary artery bypass surgery (CABG) [2]. In that case there was ST depression in I, aVL, II, aVF and V2-V6. ST elevation was 2 mm in aVR and 1 mm in V1. This patient had reported with recent onset angina.
Usually patients with LMCA occlusion deteriorate hemodynamically and electrically very rapidly [3]. They can present with anterior wall infarction. On other extreme, total left main coronary artery occlusion with normal ECG and left ventricular function has also been reported in literature [4]. In that patient, collaterals from right coronary artery supplied both left anterior descending and left circumflex coronary arteries.
Significant left coronary artery narrowing of more than 50% luminal narrowing is noted in about 5% of patients undergoing coronary angiography. But total occlusion being documented on coronary angiography is extremely rare as many of them do not survive. One series documented only 6 patients in around twelve thousand cases [5].
References
- Yamaji H, Iwasaki K, Kusachi S, Murakami T, Hirami R, Hamamoto H, Hina K, Kita T, Sakakibara N, Tsuji T. Prediction of acute left main coronary artery obstruction by 12-lead electrocardiography. ST segment elevation in lead aVR with less ST segment elevation in lead V1. J Am Coll Cardiol. 2001 Nov 1;38(5):1348-54.
- Shinde RS, Hiremath MS, Makhale CN, Durairaj M. Images in cardiology. ECG showing features of total left main coronary artery occlusion. Heart. 2006 May;92(5):670.
- Bhatia V, Parida AK, Pandey AK, Kaul U. 12 lead ECG in the detection of left main coronary artery occlusion during acute coronary syndromes. Int J Cardiol. 2007 Apr 4;116(3):e83-4.
- Singhal G, Pathak V, Mittal S. Total left main coronary artery occlusion with normal ECG and normal LV function: A rare case. Journal of Indian College of Cardiology. 2016; 6:49-51.
- Ward DE, Valantine H, Hui W. Occluded left main stem coronary artery report of five patients and review of published reports. Br Heart J. 1983;49:276–279.
Related Posts

About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal