M-Mode echocardiography and Anatomical M-Mode
M-Mode echocardiography and Anatomical M-Mode
M-Mode echocardiography (Time-motion mode) was one of the earliest tools of the echocardiographer. M-Mode gives an ice-pick view of the heart. The vertical axis gives the distance of each point from the transducer while horizontal axis gives the time period. M-Mode gives high resolution in the time axis so that it is easy to time various events in the cardiac cycle, especially if a synchronized ECG tracing is displayed along with it. One of the commonest sites of imaging is the parasternal region. As we sweep from base to apex, the initial section imaged will have the aorta anteriorly and left atrium posteriorly. The next set of images is taken at the mitral valve and another at the chordal level. Imaging at the chordal level is quite popular for taking measurements of the left ventricle in systole and diastole to calculate the ejection fraction. The thickness of the interventricular septum (IVS) and left ventricular posterior wall (LVPW) are measured at this level. Asymmetric septal hypertrophy can be seen in hypertrophic cardiomyopathy. Septum can be thinned out in anterior wall myocardial infarction, while the posterior wall will be thinned in inferoposterior infarction. Normally the septum moves with the left ventricle, meaning that it moves posteriorly in systole. Paradoxical anterior movement of septum in systole can be seen in atrial septal defect and other conditions of right ventricular volume overload. Assessment of left ventricular ejection fraction by M-Mode will be erroneous when the septal motion is paradoxical.
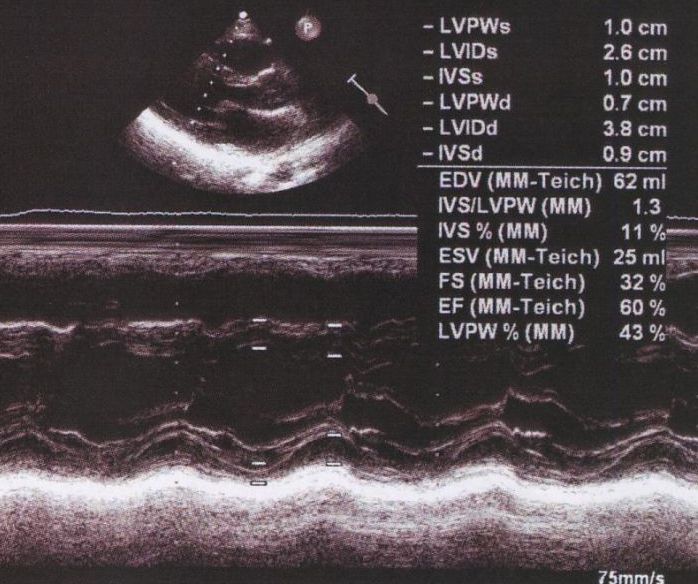
RV: right ventricle; LV: left ventricle; IVS: interventricular septum; LVPW: left ventricular posterior wall; LVIDs: left ventricular internal diameter, systolic; LVIDd: left ventricular internal diameter, diastolic
Limitation of M-Mode measurement
Accurate M-Mode measurements require good orientation of the cursor perpendicular to the long axis of the left ventricle. If the cursor orientation is oblique, measurements will be overestimated. Availability of anatomical M-Mode is useful in such situations. In anatomical M-Mode computer software makes a correction and the cursor can be manually made perpendicular to the long axis of the left ventricle.
An important use of anatomical M-Mode is the assessment of regional wall motion. It eliminates limitation due to the subjective nature of wall motion evaluation by two dimensional echocardiography [1]. Anatomical M-Mode cuts can be made in any direction and wall motion abnormalities quantified.
Reference
- Carerj S, Micari A, Trono A, Giordano G, Cerrito M, Zito C, Luzza F, Coglitore S, Arrigo F, Oreto G. Anatomical M-mode: an old-new technique. Echocardiography. 2003 May;20(4):357-61.
About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal