



Mechanical complications after an acute myocardial infarction are life-threatening events that typically occur within the first week following the insult. While their incidence has decreased significantly in the era of primary percutaneous coronary intervention (PCI), they still carry very high mortality rates. These complications generally result from the necrosis of myocardial tissue, leading to structural failure.
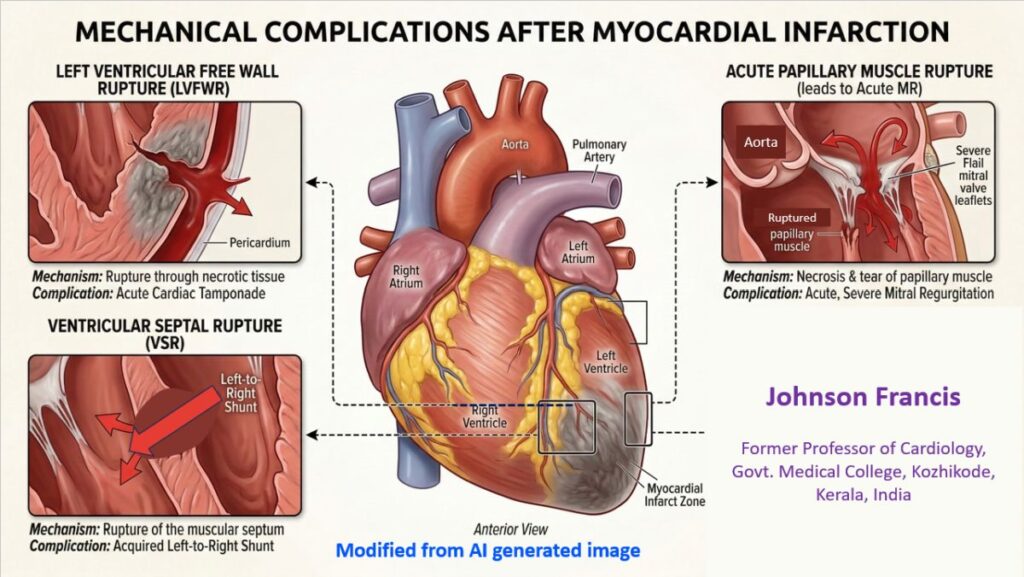
Left Ventricular Free Wall Rupture
This is the most dangerous mechanical complication, which can occur 3 to 7 days post-MI.
- Pathophysiology: Infarcted tissue becomes soft and shears under intraventricular pressure.
- Presentation: Sudden onset of pulseless electrical activity (PEA) due to acute cardiac tamponade.
- Prognosis: Often fatal within minutes. Subacute cases may form a “pseudoaneurysm” if the rupture is contained by the pericardium.
Ventricular Septal Rupture (VSR)
A rupture in the interventricular septum creates an acquired Left-to-Right shunt.
- Presentation: Sudden clinical deterioration with a new, harsh holosystolic murmur (usually at the left lower sternal border) and a palpable thrill.
- Diagnosis: Confirmed by echocardiography showing the shunt or a “step-up” in oxygen saturation from the right atrium to the right ventricle during right heart catheterization.
- Management: Requires aggressive afterload reduction followed by urgent surgical repair.
Acute Papillary Muscle Rupture
This leads to acute, severe Mitral Regurgitation (MR).
- Pathophysiology: Most commonly involves the posteromedial papillary muscle because it usually has a single blood supply (Right Coronary Artery), whereas the anterolateral muscle has dual supply (LAD and LCx).
- Presentation: Acute pulmonary edema and cardiogenic shock. A systolic murmur may be heard, but in severe cases, the murmur may be surprisingly soft due to rapid equalization of pressures between the LV and LA.
- Management: Stabilization with vasodilators or IABP, followed by emergency mitral valve replacement or repair.