


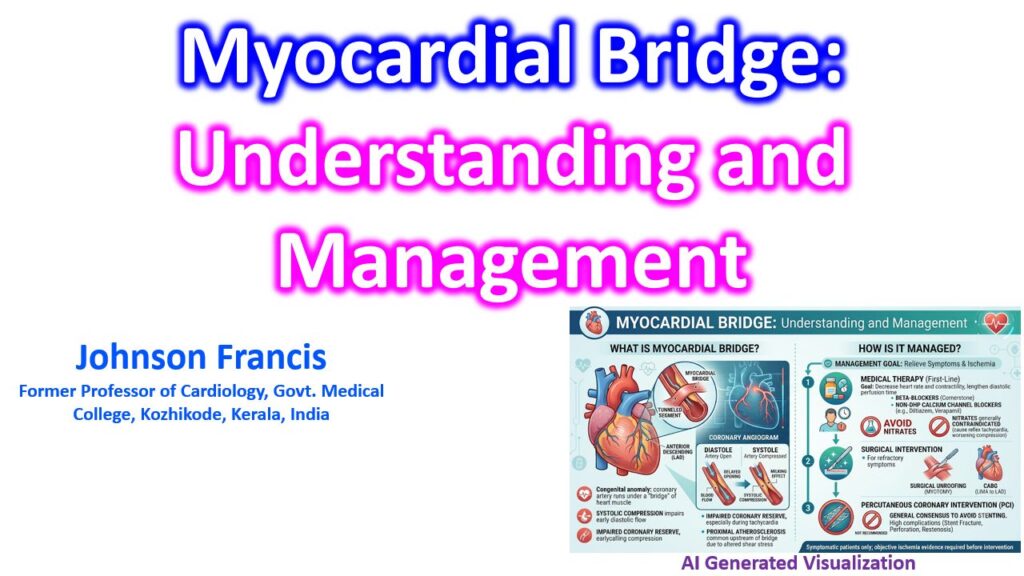

A myocardial bridge is a congenital anomaly where a segment of an epicardial coronary artery—most commonly the mid-left anterior descending (LAD) artery—dips into the myocardium and runs under a “bridge” of cardiac muscle before resurfacing. While the condition is present from birth, patients typically remain asymptomatic until their third or fourth decade of life when changes in heart rate, contractility, or the development of proximal atherosclerosis begin to restrict flow.
Pathophysiology and Hemodynamics
The clinical significance of a myocardial bridge comes down to abnormal hemodynamics rather than just the structural anomaly:
- Systolic Compression and Diastolic Delay: The overlying muscle band compresses the artery during systole (the angiographic “milking effect”). Because 80-85% of coronary blood flow occurs during diastole, this systolic compression was historically thought to be benign. However, the tunneled segment experiences a delayed reopening during early diastole, which impairs coronary reserve.
- The Tachycardia Effect: As heart rate increases (e.g., during exertion), the diastolic filling time shortens. This exacerbates the ischemia caused by the delayed early-diastolic reopening of the vessel.
- Proximal Atherosclerosis: The systolic compression creates altered shear stress and flow disturbances in the vessel segment immediately proximal to the bridge. This makes the proximal segment highly susceptible to endothelial dysfunction and accelerated atherosclerosis. Interestingly, the tunneled segment itself is usually spared from plaque formation.
Management Strategy
Treatment is reserved for symptomatic patients or those with objective evidence of ischemia (often assessed via diastolic fractional flow reserve (dFFR) or intravascular ultrasound). Asymptomatic incidental findings require no intervention.
1. Medical Therapy (First-Line)
The goal of medical management is to decrease the heart rate and reduce contractility, thereby extending diastolic perfusion time and reducing the force of the systolic compression.
- Beta-blockers: The cornerstone of therapy. Their negative chronotropic and inotropic effects directly counteract the primary mechanisms of ischemia in myocardial bridging.
- Non-dihydropyridine Calcium Channel Blockers: Agents like diltiazem or verapamil are used if beta-blockers are contraindicated or poorly tolerated, as they provide similar heart rate control.
- Avoid Nitrates: Nitroglycerin is generally contraindicated for isolated myocardial bridging. Nitrates induce reflex tachycardia and vasodilate the non-tunneled coronary segments. This effectively worsens the pressure gradient across the bridge and exacerbates the systolic compression.
2. Surgical Intervention
Surgical options are considered for patients with refractory symptoms despite maximal medical therapy and clear evidence of ischemia.
- Surgical Unroofing (Myotomy): The definitive treatment. The surgeon dissects and divides the overlying myocardial muscle band, relieving the compression.
- CABG (LIMA to LAD): Reserved for extensive, deep bridges where unroofing carries a high risk of right ventricular perforation, or when the patient has significant concomitant atherosclerotic disease proximal to the bridge.
3. Percutaneous Coronary Intervention (PCI)
Stenting a myocardial bridge is generally discouraged. Placing a rigid stent inside a vigorously contracting muscle band leads to high complication rates, including stent fracture, coronary perforation, and aggressive in-stent restenosis. It is typically only considered in highly selected cases where surgery is not an option.