



Intervention Thresholds
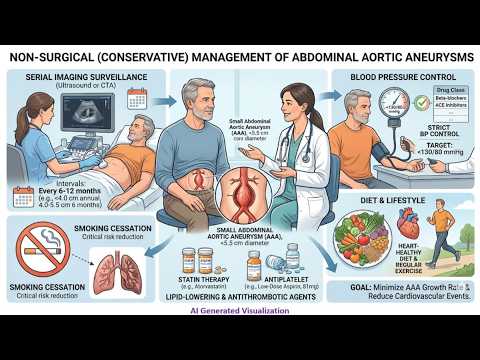
Non-surgical (Conservative) management is the standard of care for asymptomatic abdominal aortic aneurysms (AAAs) that fall below the threshold for elective repair. Intervention is typically deferred until the risk of rupture—which is remarkably low for small AAAs—outweighs the procedural risks of endovascular aneurysm repair (EVAR) or open surgery.
Elective repair is generally indicated when the AAA reaches:
- 5.5 cm in men
- 5.0 cm in women
- A rapid expansion rate of 0.5 cm or more within 6 months
Imaging Surveillance Intervals
Surveillance relies primarily on ultrasound to track the maximum anteroposterior diameter. Computed tomography angiography (CTA) is generally reserved for treatment planning once the diameter threshold has been met, or if rupture is suspected.
The 2024 European Society for Vascular Surgery (ESVS) guidelines recommend the following gender-specific screening intervals:
| Aortic Diameter | Men | Women |
| 25 to 29 mm | Every 5 years | Every 5 years |
| 30 to 39 mm | Every 3 years | Every 3 years |
| 40 to 44 mm | Annually | Annually |
| 45 to 49 mm | Annually | Every 6 months |
| 50 to 54 mm | Every 6 months (≥ 55 mm elective repair) | Repair indicated (≥ 50 mm elective repair) |
Note: ACC/AHA 2022 guidelines offer closely aligned intervals, typically recommending 3-year intervals for 3.0 to 3.9 cm, annual imaging for 4.0 to 4.9 cm, and 6-month imaging for 5.0 to 5.4 cm.
Medical and Lifestyle Management
Pharmacotherapy and lifestyle modifications focus on reducing overall cardiovascular morbidity, though no specific medication has been definitively proven to halt AAA expansion.
- Smoking Cessation: This is the most critical modifiable risk factor. Continued smoking is directly correlated with accelerated expansion rates and a significantly higher risk of rupture.
- Cardiovascular Risk Reduction: Standard secondary prevention protocols apply, requiring strict blood pressure control, high-intensity statin therapy, and antiplatelet therapy.
- Physical Activity: Routine exercise do not need to be restricted in patients with small, asymptomatic AAAs.
- Fluoroquinolones: While the FDA previously issued warnings regarding fluoroquinolone use in patients with aortic disease, the 2024 ESVS guidelines clarify that a small AAA is not a strict contraindication if these antibiotics are otherwise clinically necessary.