



Paroxysmal Nocturnal Dyspnea (PND) is a cardinal symptom of left ventricular decompensation. While often grouped with orthopnea, its underlying biophysical triggers and delayed onset during sleep make it a distinct—and highly specific—clinical marker for elevated left-sided filling pressures.
Here is a breakdown of the hemodynamic mechanisms and clinical implications of PND.
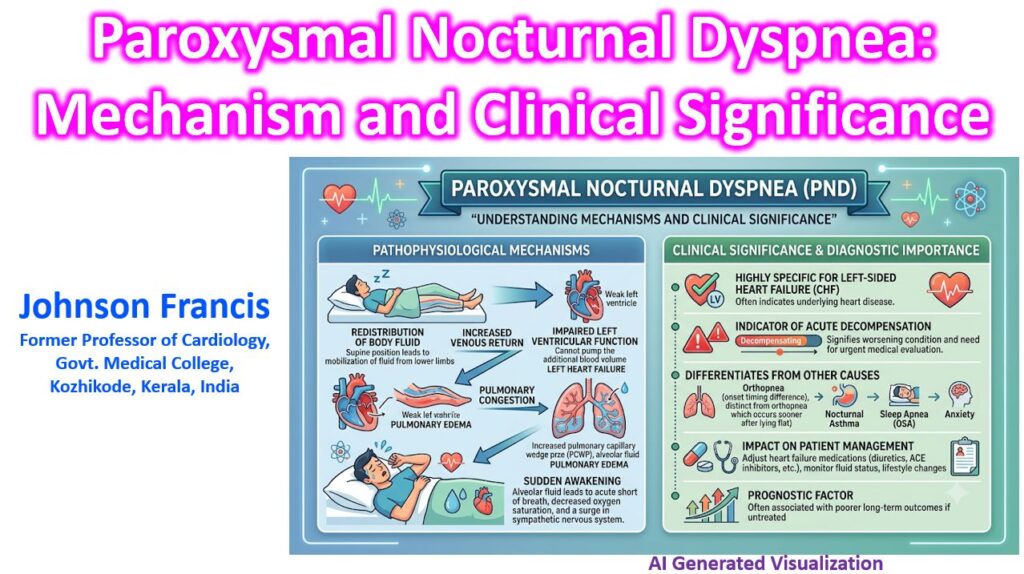
Pathophysiological Mechanisms
The onset of PND is driven by a complex interplay of postural fluid shifts, ventricular mismatch, and sleep physiology, typically occurring 2 to 4 hours after falling asleep.
1. The Preload Surge (Fluid Redistribution)
When a patient transitions from an upright to a supine position, gravity ceases to pool blood in the lower extremities and splanchnic bed. The gradual mobilization of dependent interstitial edema increases central venous return. The right ventricle pumps this augmented volume into the pulmonary circulation.
2. Left Ventricular Mismatch
In the setting of left ventricular (LV) systolic dysfunction or reduced compliance (HFpEF), the LV cannot accommodate the increased pulmonary venous return.
- This creates an acute hemodynamic bottleneck.
- Left Ventricular End-Diastolic Pressure (LVEDP) and Left Atrial (LA) pressure rise significantly, directly transmitting retrograde hydrostatic pressure to the pulmonary capillaries.
3. Starling Forces and Transudation
The accumulation of fluid in the pulmonary interstitium is governed by Starling’s law of the capillaries:
Jv = Kc [(Pc – Pi) – σ (πc – πi)]
Where capillary hydrostatic pressure (Pc) drastically exceeds plasma oncotic pressure (πc). The resulting fluid transudation thickens the alveolar-capillary membrane, decreasing pulmonary compliance and impairing gas exchange (causing hypoxemia).
4. The Sleep Physiology Component
Unlike orthopnea, which occurs within minutes of lying down, PND is delayed. During sleep, central respiratory drive is depressed, and sympathetic nervous system tone decreases.
- The blunted adrenergic response prevents the heart from increasing contractility to handle the preload surge.
- The reduced sensitivity of the respiratory center to mild hypoxemia allows pulmonary congestion to silently accumulate until a critical threshold is reached. The patient is then abruptly awakened by severe air hunger, tachypnea, and sympathetic surge.
Clinical Significance
Identifying true PND is critical for differential diagnosis and risk stratification in cardiology and internal medicine.
High Specificity for Left Heart Failure
While dyspnea is a broad symptom, PND is highly specific for congestive heart failure.
| Condition | Timing of Onset | Relief Mechanism | Hallmark Feature |
| PND | 2–4 hours after sleep | Sitting upright for 15–30 mins | Abrupt awakening, severe air hunger, coughing. |
| Orthopnea | < 5 mins of lying flat | Sitting upright immediately | Predictable positional intolerance. |
| OSA | Intermittent throughout sleep | Brief arousal / CPAP | Snoring, witnessed apneas, daytime somnolence. |
| Asthma (Nocturnal) | Early morning (circadian dip) | Bronchodilators | Wheezing, chest tightness, unrelated to posture. |
Prognostic Indicator
The presence of PND indicates that the patient has exhausted their compensatory mechanisms. It is a sentinel marker of impending acute decompensated heart failure (ADHF). A patient reporting new or worsening PND requires immediate re-evaluation of their volume status and rapid optimization of their diuretic regimen or afterload-reducing agents.
The “Cardiac Asthma” Mimic
Because the interstitial edema of PND can compress small bronchioles, patients may present with wheezing rather than classic crackles. This “cardiac asthma” is frequently misdiagnosed as an exacerbation of COPD or late-onset asthma, leading to inappropriate treatment with beta-agonists (which may provoke arrhythmias) rather than loop diuretics.