


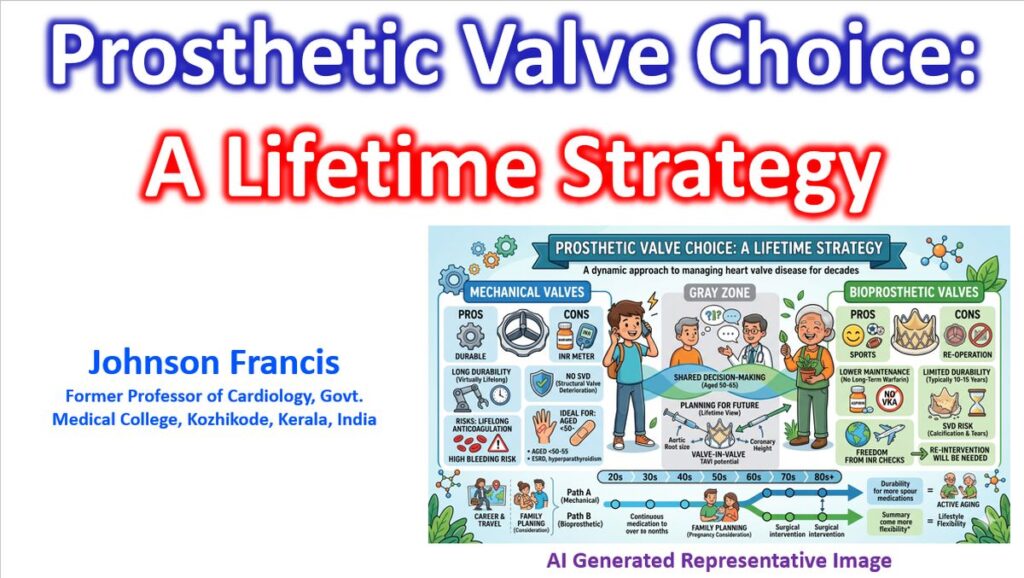

The choice between a mechanical and a bioprosthetic valve is increasingly viewed through the lens of “lifetime management,” shifting away from a simple age-based binary toward a more nuanced assessment of patient longevity, lifestyle, and the feasibility of future interventions. Current guidelines emphasize shared decision-making, but several objective clinical pillars remain central to the selection process.
1. Mechanical Prostheses
Mechanical valves are generally favored when durability is the primary concern and the patient can safely manage long-term anticoagulation.
- Durability: Virtually lifelong; the risk of structural valve deterioration (SVD) is negligible.
- Anticoagulation: Requires lifelong Vitamin K Antagonists (VKA), usually with a target INR of 2.0–3.0 for aortic positions and 2.5–3.5 for mitral positions.
- Ideal Candidate:
- Patients aged <50 (Aortic) or <55 (Mitral).
- Patients already on anticoagulation for other reasons (e.g., Atrial Fibrillation).
- Patients with a high risk of rapid bioprosthetic calcification (e.g., end-stage renal disease or hyperparathyroidism).
According to a comparative study published in NEJM in 2017, long-term mortality benefit associated with a mechanical prosthesis, as compared with a biologic prosthesis, persisted until 70 years of age among patients undergoing mitral-valve replacement and until 55 years of age among those undergoing aortic-valve replacement.
2. Bioprosthetic (Tissue) Valves
Bioprosthetic valves are selected to avoid the lifestyle constraints and bleeding risks associated with warfarin, acknowledging that a re-intervention will likely be necessary.
- Durability: Limited by Structural Valve Degeneration (SVD), which typically occurs 10–15 years post-implantation, though newer generation valves may offer improved longevity.
- Anticoagulation: Only required for the first 3–6 months post-operatively (aspirin or VKA), unless other indications exist.
- Ideal Candidate:
- Patients aged >65–70.
- Patients with contraindications to long-term anticoagulation or high bleeding risk.
- Women planning pregnancy (to avoid the teratogenicity of warfarin).
- Patients whose lifestyle or occupation makes anticoagulation dangerous (e.g., contact sports, manual labor).
3. The “Gray Zone” and Lifetime Strategy
For patients aged 50 to 65, the decision is highly individualized. The focus has shifted toward the “Valve-in-Valve” (ViV) potential.
- Aortic Position: If a bioprosthesis is chosen in a younger patient, the surgeon must consider the sinus of Valsalva anatomy and coronary height to ensure a future TAVI (Transcatheter Aortic Valve Implantation) is technically feasible.
- Small Annulus: In patients with a small aortic root, a mechanical valve or a root enlargement procedure may be preferred to avoid Prosthesis-Patient Mismatch (PPM), which significantly impacts long-term survival.
4. Summary of Clinical Considerations
| Factor | Mechanical | Bioprosthetic |
| Durability | Excellent (>25+ years) | Limited (10–15 years) |
| Thromboembolism | Higher risk | Lower risk |
| Anticoagulation | Lifelong Warfarin (INR monitoring) | Short-term or None |
| Re-operation | Rare | Likely in younger patients |
| Infective Endocarditis | Higher morbidity | Slightly better salvage potential |
5. Emerging Trends
- TAVI vs. SAVR: The expansion of TAVI into lower-risk and younger populations is influencing the initial choice of a surgical bioprosthesis, with many clinicians opting for “TAVI-friendly” surgical valves to simplify future transcatheter redo procedures.
- On-X Valves: These newer mechanical valves allow for lower INR targets (1.5–2.0 for aortic) after the initial three months, potentially reducing the bleeding burden of traditional mechanical options.