



Pulsed Field Ablation (PFA) has emerged as a revolutionary paradigm shift in the treatment of atrial fibrillation (AF), transitioning with unprecedented speed from an experimental concept to a mainstream standard of care in electrophysiology labs worldwide. I am glad that the first one in my region has been performed right in my city! Unlike traditional thermal ablation modalities—such as Radiofrequency (RF) ablation (heat) and Cryoablation (cold)—PFA relies on a non-thermal energy mechanism called irreversible electroporation (IRE).
⚡ Mechanism of Action: Irreversible Electroporation
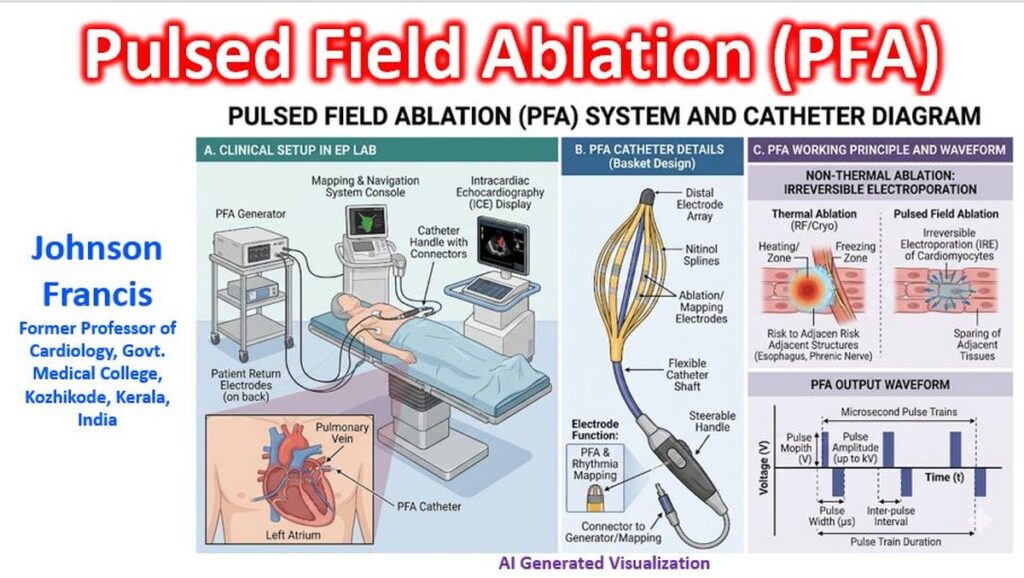
PFA utilizes ultrashort (microsecond or nanosecond), high-voltage electrical fields to target cardiac tissue.
- Cellular Disruption: These electrical pulses disrupt the lipid bilayer of cell membranes, creating permanent nanopores. This leads to a loss of cellular homeostasis, leaking of vital ions, and subsequent apoptosis or necrosis of the tissue.
- Tissue Selectivity: The primary clinical advantage of PFA is its high threshold selectivity. Cardiomyocytes have a significantly lower electrical field threshold for cell death compared to adjacent non-cardiac structures. This means the ablation can successfully isolate pulmonary veins while leaving vulnerable neighboring tissues unharmed.
🏆 Key Advantages Over Thermal Ablation
Traditional thermal therapies can cause collateral damage due to heat or cold dissipation. PFA addresses these critical limitations by offering:
- Unmatched Safety Profile: Because it preserves the extracellular matrix and selectively spares non-cardiac tissue, PFA drastically reduces or eliminates catastrophic complications like atrio-esophageal fistulas, phrenic nerve paralysis, and pulmonary vein stenosis.
- Procedural Efficiency: PFA lesions are created in a fraction of a second compared to the tens of seconds required for a single thermal application. Landmark trials show that total pulmonary vein isolation (PVI) time and left atrial dwell time are significantly reduced, optimizing laboratory workflows.
- High Efficacy and Lesion Durability: Advanced multielement or “single-shot” conformable lattice catheters allow operators to achieve rapid, contiguous lesions with high acute success rates and excellent long-term durability upon remapping.
📊 Clinical Evidence & Trials
Major global multi-center trials have solidified PFA’s place in clinical guidelines:
| Trial / Registry | Focus & Findings |
| ADVENT Trial | The definitive prospective, randomized controlled trial demonstrating that PFA is non-inferior to conventional thermal ablation (RF and Cryo) regarding primary safety and efficacy endpoints in paroxysmal AF, with a lower rate of redo ablations. |
| MANIFEST-17K | A massive real-world post-market registry tracking over 17,000 patients, confirming excellent safety and reproducibility across diverse global centers. |
| Sphere-360 Trials | Evaluating newer “all-in-one” single-shot mapping and ablation lattice catheters, showing a 1-year freedom from atrial arrhythmias of up to 88% with highly optimized pulse waveforms. |
⚠️ Emerging Challenges and Nuances
While PFA has revolutionized the field, widespread clinical implementation has revealed unique challenges that require careful management:
- Hemolysis and Renal Strain: The high-voltage electrical fields cause mechanical destruction of red blood cells (hemolysis) passing through the catheter array. Severe or excessive ablation can lead to high free plasma hemoglobin and myoglobin levels, which are nephrotoxic and have occasionally caused acute kidney injury requiring temporary dialysis. Post-procedural hydration protocols are frequently utilized to mitigate this risk.
- Microbubble Formation & Coronary Spasm: Rapid electrical arcs can generate transient microbubbles in the bloodstream or induce localized, temporary coronary artery vasospasms, particularly when ablating near the mitral annulus or tricuspid isthmus.
- Skeletal Muscle Activation: PFA requires general anesthesia or deep sedation because the high-voltage pulses stimulate skeletal muscle contraction, requiring adequate neuromuscular blockade for patient safety and comfort.
🔮 Current Outlook
According to consensus surveys by the European Heart Rhythm Association (EHRA), PFA has reshaped electrophysiology, capturing a dominant share of first-time PVI procedures over the last few years. The field is currently transitioning into an integrated workflow era, where single-catheter designs combine high-density electroanatomical mapping with immediate pulsed-field delivery, creating a highly customized, fast, and safe approach to conquering atrial fibrillation.
Short video clips of the procedure are available at the X handle of @DrArunGopi1: https://x.com/DrArunGopi1/status/2063216365792891375
References
- Francis J. Pulsed Field Ablation for Atrial Fibrillation. BMH Med. J. 2025; 12(2): 14-16.
- Bergonti M, Mills MT, Roten L, Ruwald MH, Metzner A, Conte G, Zylla MM, Vlachos K, Mazurek M, Perrotta L, Futyma P, Sultan A, Heeger CH, Chun JKR. Pulsed field ablation for atrial fibrillation ablation: a European Heart Rhythm Association survey. Europace. 2025 Dec 1;27(12):euaf294. doi: 10.1093/europace/euaf294. PMID: 41363248; PMCID: PMC12686987.
- Koniari I, Artopoulou E, Gall S, Chu GS, Koros R, Bozika M, Nastouli KM, Leventopoulos G, Chalil S, Arujuna A. Pulsed Field Ablation for Atrial Fibrillation: Contemporary Clinical Evidence and Real-World Experience in Redo Ablation. J Clin Med. 2026 Feb 22;15(4):1647. doi: 10.3390/jcm15041647. PMID: 41753335; PMCID: PMC12941725.
- Pürerfellner H, Merino JL, Burri H, Boriani G, Kühne M. Pulsed field ablation: from technological breakthrough to structured clinical implementation-the role of the European Heart Rhythm Association. Europace. 2026 Mar 30;28(4):euag074. doi: 10.1093/europace/euag074. PMID: 41968952; PMCID: PMC13122612.
- Reddy VY, Peichl P, Kautzner J, Anter E, Metzner A, Koruth J, Jais P, Rackauskas G, Petru J, Funasako M, Marinskis G, Turagam M, Aidietis A, Selma JM, Nejedlo V, Kueffer F, Tarakji KG, Natale A, Neuzil P. One-year outcomes of a conformable single-shot pulsed-field ablation catheter for the treatment of paroxysmal atrial fibrillation. Heart Rhythm. 2025 Oct;22(10):2551-2561. doi: 10.1016/j.hrthm.2025.04.031. Epub 2025 Apr 26. PMID: 40294729.
- Tzeis, S., Gerstenfeld, E. P., Kalman, J., Saad, E. B., Shamloo, A. S., Andrade, J. G., Barbhaiya, C. R., Baykaner, T., Boveda, S., Calkins, H., Chan, N.-Y., Chen, M., Chen, S.-A., Dagres, N., Damiano, R. J., De Potter, T., Deisenhofer, I., Derval, N., Di Biase, L., Duytschaever, M., Dyrda, K., Hindricks, G., Hocini, M., Kim, Y.-H., & la Meir, M. (2024). 2024 European Heart Rhythm Association/Heart Rhythm Society/Asia Pacific Heart Rhythm Society/Latin American Heart Rhythm Society expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm, 21, e31–e149. https://doi.org/10.1016/j.hrthm.2024.03.017
Cited by: 762 - Vázquez-Calvo S, Poletaev V, Verma A. Latest Advances and Ongoing Challenges in Pulsed Field Ablation. Arrhythm Electrophysiol Rev. 2026 Feb 24;15:e06. doi: 10.15420/aer.2025.32. PMID: 41835109; PMCID: PMC12983143.
- Ye J, Fan Y, Wang Y, Jian Y, Gao Y, Chen S, Xuan J, Hu H. Health economic analysis of pulsed field ablation compared to conventional thermal ablation for patients with paroxysmal atrial fibrillation in China. J Comp Eff Res. 2026 May;15(5):e250153. doi: 10.57264/cer-2025-0153. Epub 2026 Apr 29. PMID: 42052747; PMCID: PMC13154590.