Right bundle branch block with right upper quadrant axis
Right bundle branch block with right upper quadrant axis
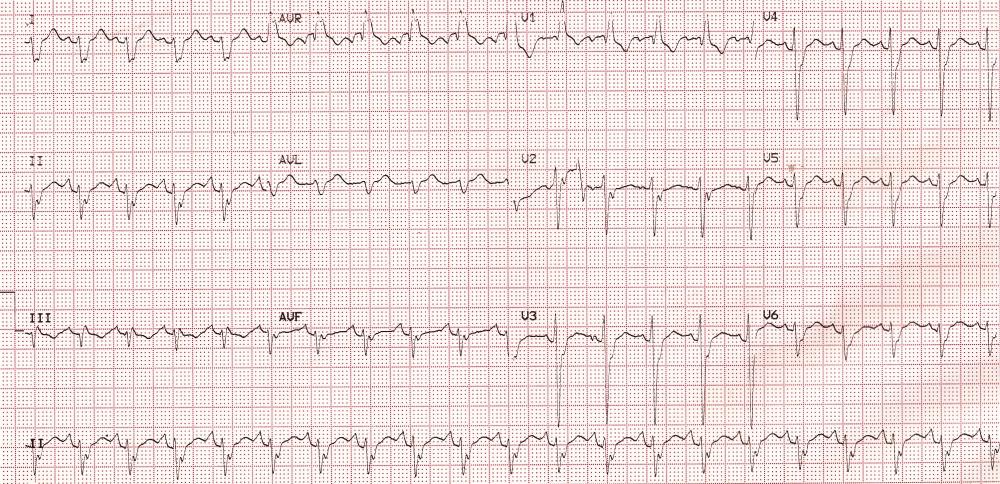
ECG demonstrating right bundle branch block with right upper quadrant axis: rsR’ pattern in V1, rS pattern in I, aVL and V6 are all features of right bundle branch block (RBBB). The amplitude of r waves in lateral leads are quite low. QRS width is a little more than 120 ms. The QRS axis is in the North West region (right upper quadrant), which can mean either extreme right axis or extreme left axis deviation. rS pattern is seen both in inferior leads and in lateral leads. Hence it is rather difficult to say whether it is left anterior hemiblock (LAHB) or left posterior hemiblock (LPHB) which is associated with the RBBB. PR interval is normal. Hence it can be considered as bifascicular block. QRS pattern in chest leads show a clockwise rotation with S waves persisting up to V6. The slurred R’ in V1 and slurred S waves in lateral leads suggest delayed activation of the right ventricular myocardium which proceeds by conduction through the myocardium rather than through the specialized conduction system of the heart.
Right upper quadrant or North West QRS axis
North West axis has been reported in flecainide toxicity [1]. In those with QRS width 200 ms or less right bundle branch block pattern was more likely. In those with QRS duration above 200 ms, ECG was more likely to show left bundle branch block pattern and North West axis.
In another study, it has been shown that in patients late after repair of tetralogy of Fallot with significant pulmonary regurgitation, QRS duration of 150 ms or more and North West quadrant QRS axis can predict marked right ventricular enlargement [2]. That study had evaluated 20 patients with magnetic resonance imaging for measurement of right ventricular volume. They had enlarged and hypokinetic right ventricles by echocardiography.
In a case report of North West QRS axis in a patient presenting with chest pain, it was due to acute inferoposterolateral myocardial infarction [3]. North West axis has been noted in idiopathic left ventricular tachycardia [4]. That 15 year old male had multiple emergency room visits with wide QRS complex tachycardia having right bundle branch block (RBBB) morphology and North West axis. Ventricular tachycardia with RBBB pattern and North West axis can also occur in hypertrophic cardiomyopathy [5,6].
North West QRS axis is noted in biventricular pacing with right ventricular pacing at the apex. When the right ventricular pacing is from the outflow region, the QRS axis is often in the right inferior quadrant. North West axis may be rarely seen in left ventricular pacing and right ventricular apical pacing, though these are not the usual pattern in these pacing locations [7].
References
- Valentino MA, Panakos A, Ragupathi L, Williams J, Pavri BB. Flecainide Toxicity: A Case Report and Systematic Review of its Electrocardiographic Patterns and Management. Cardiovasc Toxicol. 2017 Jul;17(3):260-266.
- Book WM, Parks WJ, Hopkins KL, Hurst JW. Electrocardiographic predictors of right ventricular volume measured by magnetic resonance imaging late after total repair of tetralogy of Fallot. Clin Cardiol. 1999 Nov;22(11):740-6.
- Glancy DL, Staggs SE, Irimpen AM, Hardwick JC 3rd. ECG of the month. Chest pain and a northwest QRS axis. Acute inferoposterolateral myocardial infarction. J La State Med Soc. 2002 Sep-Oct;154(5):219-20.
- Weng KP, Chiou CW, Kung MH, Lin CC, Hsieh KS. Radiofrequency catheter ablation of coexistent idiopathic left ventricular tachycardia and atrioventricular nodal reentrant tachycardia. J Chin Med Assoc. 2005 Oct;68(10):479-83.
- Okumura Y, Watanabe I, Ohkubo K, Saito S. Successful catheter ablation for incessant ventricular tachycardia in a patient with hypertrophic cardiomyopathy. Circ J. 2007 Jul;71(7):1164-8.
- Rodriguez LM, Smeets JL, Timmermans C, Blommaert D, van Dantzig JM, de Muinck EB, Wellens HJ. Radiofrequency catheter ablation of sustained monomorphic ventricular tachycardia in hypertrophic cardiomyopathy. J Cardiovasc Electrophysiol. 1997 Jul;8(7):803-6.
- Barold SS, Herweg B, Giudici M. Electrocardiographic follow-up of biventricular pacemakers. Ann Noninvasive Electrocardiol. 2005 Apr;10(2):231-55.
Related Posts

About The Author
Johnson Francis
Former Professor of Cardiology, Calicut Govt. Medical Kozhikode, Kerala, India. Editor-in-Chief, BMH Medical Journal