


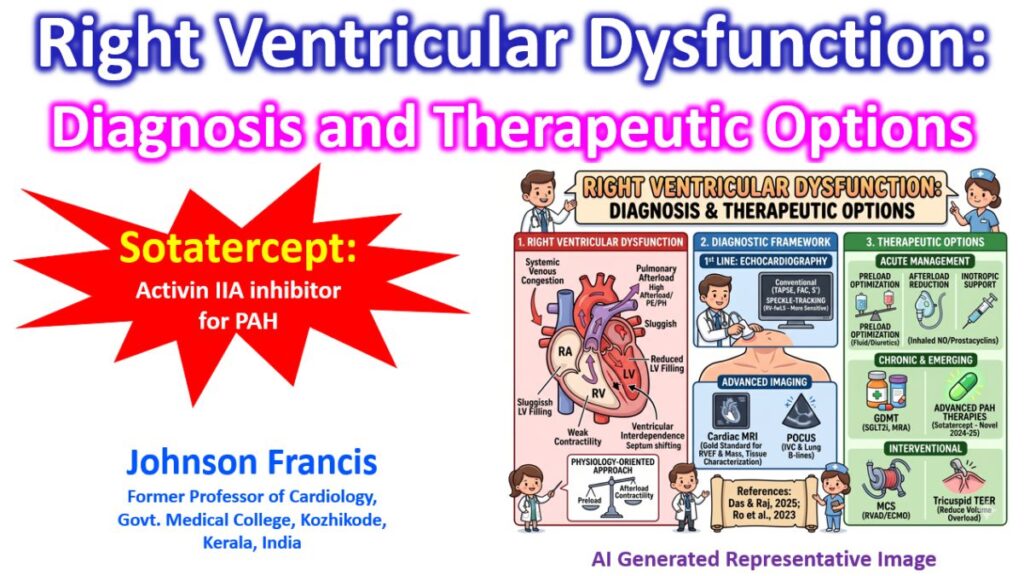

Right ventricular (RV) dysfunction is a clinical and hemodynamic syndrome resulting from impaired RV filling or ejection, often leading to systemic venous congestion and low cardiac output. Contemporary management focuses on a physiology-oriented approach that balances preload optimization, afterload reduction, and enhancement of myocardial contractility.
Diagnostic Framework
The diagnosis of RV dysfunction has transitioned from simple visual estimation to quantitative multi-modality imaging and bedside assessment.
1. First-Line Imaging: Echocardiography
Echocardiography remains the primary diagnostic tool due to its accessibility and comprehensive hemodynamic data.
- Conventional Parameters: Tricuspid Annular Plane Systolic Excursion (TAPSE), Fractional Area Change (FAC), and Doppler-derived S’ wave are standard for assessing longitudinal and global function.
- Speckle-Tracking Echocardiography (STE): Right ventricular free-wall longitudinal strain (RV-fwLS) is more sensitive than RVEF or TAPSE for detecting subclinical dysfunction and predicting clinical outcomes.
- 3D Echocardiography: Provides a more accurate quantification of RV volumes and ejection fraction (RVEF) without the geometric assumptions required by 2D imaging.
2. Advanced Modalities
- Cardiac Magnetic Resonance (CMR): The gold standard for quantifying RV mass, volumes, and RVEF. It is particularly valuable for identifying infiltrative diseases (e.g., amyloidosis) and tissue characterization.
- Point-of-Care Ultrasound (POCUS): Rapid bedside assessment of the inferior vena cava (IVC) and lung B-lines (indicating congestion) allows for real-time monitoring of therapeutic response and volume status.
Therapeutic Options
Therapeutic strategies are dictated by the chronicity of the failure and the underlying etiology, specifically focusing on the RV-PA (Pulmonary Artery) Coupling.
1. Acute Management Principles
Management of acute RV failure aims to restore systemic perfusion and prevent a “downward spiral” of ischemia and worsening afterload.
- Preload Optimization: Judicious fluid management is critical. While volume resuscitation is indicated in hypovolemia, excessive fluids in a dilated RV can cause “ventricular interdependence,” where the interventricular septum shifts leftward, reducing left ventricular (LV) filling.
- Afterload Reduction: In acute pulmonary embolism or pulmonary hypertension (PH), reducing pulmonary vascular resistance (PVR) is essential. Options include inhaled nitric oxide or prostacyclins.
- Inotropic Support: Dobutamine or milrinone may be used to enhance contractility, though care must be taken to avoid systemic hypotension.
2. Chronic Management & Emerging Therapies
- Guideline-Directed Medical Therapy (GDMT): While traditionally focused on the left heart, recent evidence supports the use of Sodium-Glucose Cotransporter-2 inhibitors (SGLT2i) and mineralocorticoid receptor antagonists (MRAs) for overall heart failure management, which may indirectly benefit RV function through improved LV hemodynamics.
- Advanced PAH Therapies: Novel agents like sotatercept (an activin signaling inhibitor) have shown significant promise in recent trials (STELLAR and ZENITH) for reducing PVR and improving RV-PA coupling in pulmonary arterial hypertension.
- Mechanical Circulatory Support (MCS): For refractory RV failure, temporary RV assist devices (RVADs) or extracorporeal membrane oxygenation (ECMO) are utilized as a bridge to recovery or transplantation.
3. Interventional Strategies
- Valvular Correction: Transcatheter edge-to-edge repair (TEER) for severe tricuspid regurgitation is increasingly used to reduce chronic volume overload on the RV.
STELLAR Trial
The pivotal Phase 3 STELLAR trial was the foundation for the FDA’s approval of sotatercept on March 26, 2024. The study demonstrated that adding sotatercept to background therapy significantly improved 6-minute walk distance (6MWD) and reduced the risk of death or clinical worsening.
Presented and published in early 2025, the ZENITH trial specifically targeted high-risk PAH patients (those on maximal therapy with a high mortality risk). The trial was stopped early due to overwhelming efficacy.
Sotatercept: The First FDA-Approved Activin A Receptor IIA Inhibitor
As mentioned, Sotatercept has been shown to improve 6 minute walk distance in patients with PAH at 24 weeks. More studies are needed to assess the mortality benefit. Currently the limitations are the high cost and unknown long-term effects. Adverse effects noted in the trials were epistaxis, telangiectasia, increased hemoglobin, hematocrit, red blood cell levels, and dizziness, compared to placebo.